


by Sara Gottfried, MD and Bianca Garilli, ND, IFMCP
Introduction
We’re just starting to understand the full spectrum of toxic threats to the human body, including obesity. What’s clear is that the body doesn’t know what to do with our myriad exposures to toxins. They clog the liver, then get stored in fat, and ultimately back up into the brain. Since the brain is almost two-thirds fat (the fattiest organ in the body), it makes sense that it’s likely the most vulnerable. In fact, the brain is the most calorie-hungry (in scientific terms, “metabolically active”) organ: It is only 2 to 3% of total body weight, but consumes 25% of total body glucose and 20% of total body oxygen. Basically, the brain is a metabolic hog.
Due to the fact that the brain uses so much of the body’s resources, it is quite vulnerable to any toxins that lower metabolism. These include obesogens—that is, foreign chemicals that lead to unwanted weight gain, disrupt insulin and other metabolic hormones, and put our patients at greater risk for obesity. Ironically, when you burn fat or lose weight, cells can release the toxins they store into the bloodstream, ready to once again tire out the mitochondria or block hormone receptors like insulin or leptin—making you hungrier and storing more fat than you burn as your liver works to recapture the freed toxins.
How do obesogens make you fat? Here’s an example: the toxin bisphenol A (BPA) found in certain plastics and resins stimulates the pancreatic beta cells, the ones that make insulin. This disturbs insulin messaging in the liver, fat, and muscle cells, ultimately leading to pancreatic dysfunction, insulin resistance, and rising blood sugar.
Obesogens—a brief history lesson
We developed our understanding of obesogens almost accidentally over the past two decades with contributions from various scientists and fields of study. As Jerrold Heindel, PhD, the Scientific Program Administrator of the National Institute of Environmental Health Sciences, noted in a recent article, it was certain out-of-the-box thinkers who were in the right place at the right time and were able to start piecing together the various data points associating environmental chemicals and weight gain that led to the breakthrough scholarship on obesogens.1
Nearly 20 years ago, Paula Baillie-Hamilton, MB, BS, DPhil, a UK physician who had gained unexplained weight after her second child, published a review article with her thoughts and findings on the possible connection between the rising levels of toxins that had flooded the global environment after World War II and the dramatic increase in weight problems throughout the country which she herself had personally experienced.2 She wrote in her landmark article, “Therefore it can be posited that the relatively recent presence of synthetic chemicals in the environment may be a significant causative factor in the current worldwide obesity epidemic. These chemicals may be causing weight gain via toxic effects on the body’s natural weight-control mechanisms.”2
It took several years and the influence of other researchers and clinicians citing her publication before this groundbreaking hypothesis caught mainstream researchers’ attention. This delay may have been because Baillie-Hamilton’s original publication was printed in the Journal of Alternative and Complementary Medicine,1 a new and relatively fringe journal at the time.
Ultimately, other scientists connected the dots of emerging research, leading to the next key publication in 2006,3 when Bruce Blumberg, PhD, now Professor of Developmental and Cell Biology and Professor of Pharmaceutical Sciences at the University of California, Irvine,4 coined the term “obesogen,” defined as, “molecules that inappropriately regulate lipid metabolism and adipogenesis to promote obesity.”3 Blumberg found that tributyltin (TBT), a member of the organotin compound group—used in agriculture and industry worldwide as biocides, heat stabilizers, and chemical catalysts—could lead to weight gain in mice.1,3 More recent work suggests that chronic and repeat exposure to low doses of TBT in male mice may lead to insulin and leptin resistance, as well as obesity and hepatic steatosis.5
Preclinical findings showing that mice exposed to endocrine-disrupting chemicals (EDCs) experienced subsequent weight gain was a turning point that helped to unite two relatively unrelated fields—EDCs and the developmental origins of health and disease (DOHaD) field, resulting in the new field of obesogens.1
Obesogens—what we know now
Although still in the learning-to-crawl stage, obesogen research has grown by leaps and bounds. The link between EDCs in general and their effects on weight gain is gaining clarity through results from both preclinical and clinical studies.1 It is now thought that exposure to EDCs during early human development is associated with increased susceptibility to many chronic health problems today including the following: infertility, asthma, breast and prostate cancers, early puberty, susceptibility to infections, heart disease, autoimmune disease, and learning disabilities like attention deficit hyperactivity disorder (ADHD).1
As the breadth of research grows, it has become apparent that obesogens have various possible mechanistic pathways through which these compounds can influence weight gain including:6,7
- Disrupting sex steroid signaling by estrogenic and/or androgenic modulation
- Influencing thyroid hormone signaling
- Disturbing metabolic pathways
- Mediating mitochondrial dysfunction
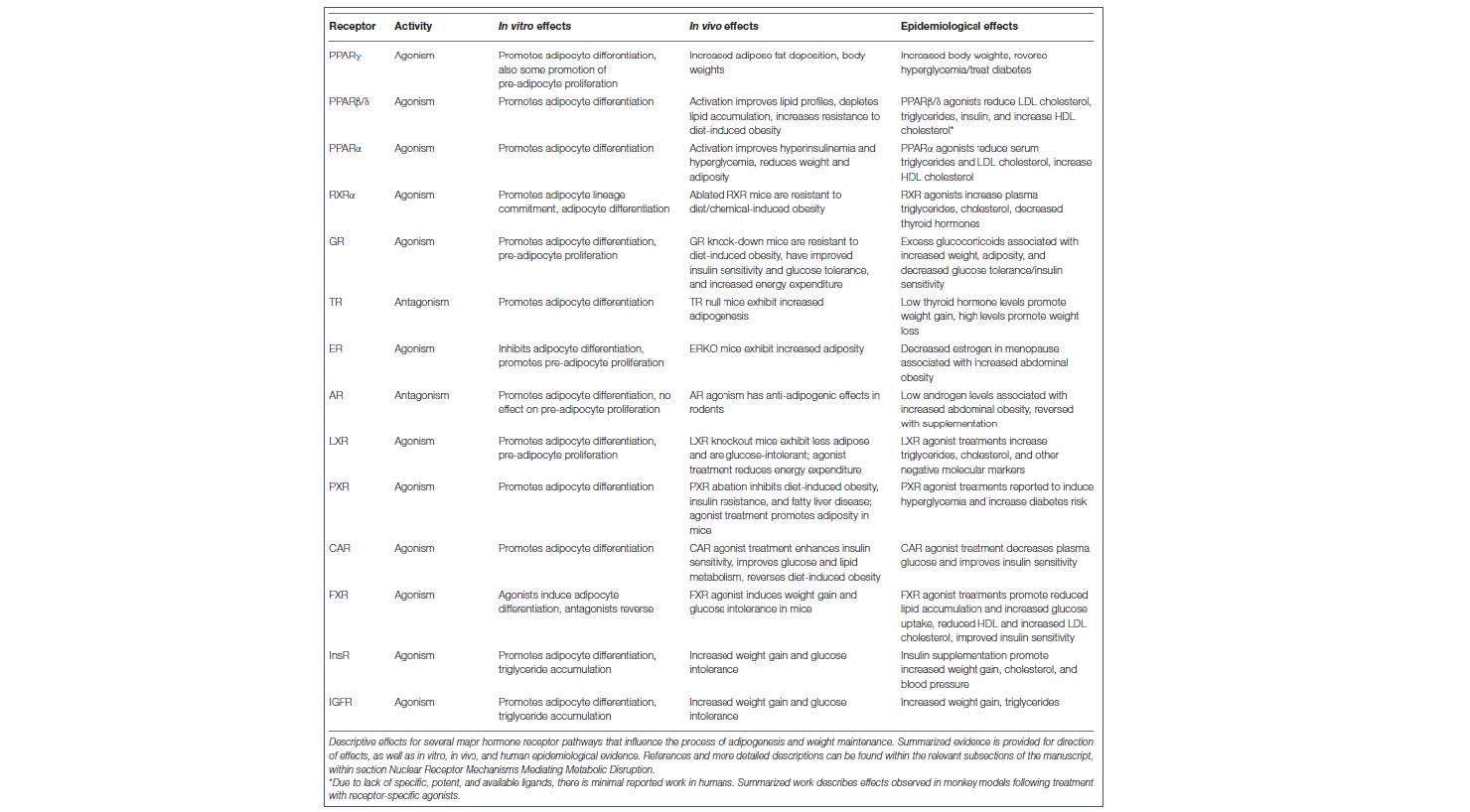
If we consider in vitro, in vivo, and human evidence of major hormone receptor pathways capable of promoting adipogenesis, it becomes clear that obesogens have the potential to impact many possible pathways (see Table 1).6
Table 1: Major hormone receptor pathways capable of promoting adipogenesis6
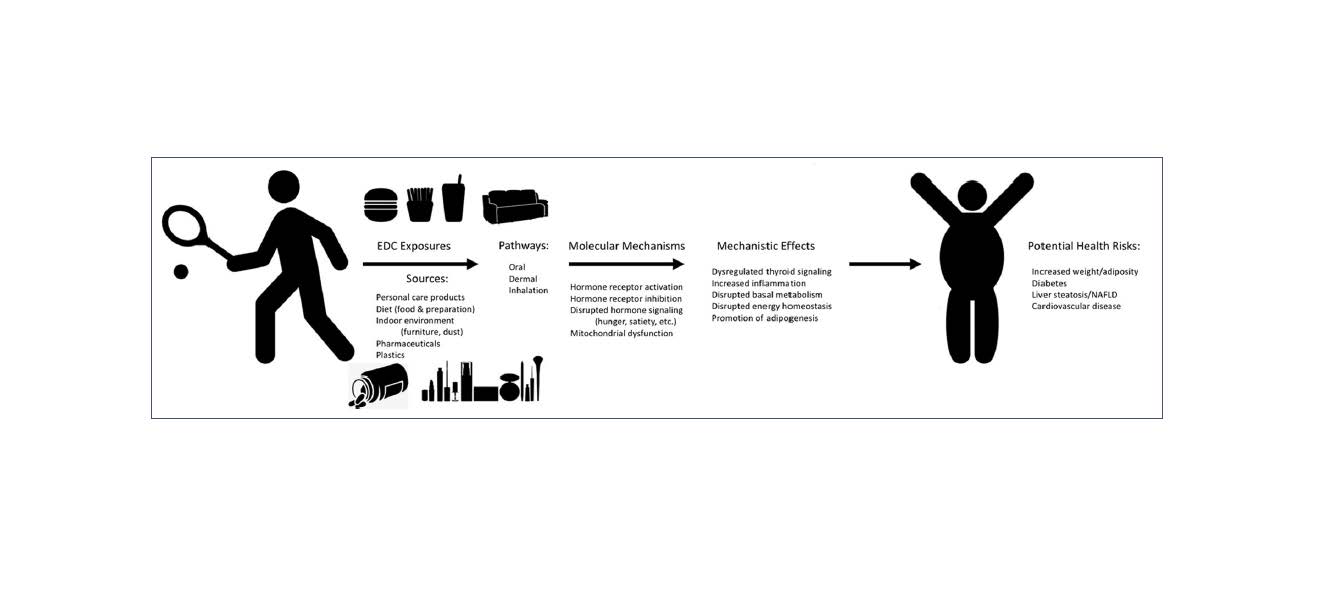
Downstream effects of EDC exposure have the potential to impact not only adipogenesis, but other processes such as inflammation, basal metabolism, and energy homeostasis, all of which are players in weight management and obesity (see Figure 1). These physiologic perturbations can then contribute to the rising rates of type 2 diabetes (T2D), cardiovascular disease (CVD), liver steatosis, and nonalcoholic fatty liver disease (NAFLD).6,8
Figure 1: Mechanisms of EDC exposure and potential human metabolic effects6
Global perspective on obesity
Prevalence rates of overweight and obesity have hit a record high across the globe, with an estimated 38% of the world’s adult population overweight and another 20% with obesity by the year 2030 if current trends continue.9 In the United States, the statistics are more grim, with projections indicating 85% of adults will meet criteria for overweight or obese categories by the same year.10
Obesity, beyond creating many physical and potentially emotional, social, and professional challenges, also greatly increases the risk of developing a multitude of chronic diseases including depression, T2D, CVD, stroke, gallbladder disease, osteoarthritis, pain, and certain cancers; Obesity also increases the risk of disability and mortality.11-13
Younger generations have not been spared, with a dramatic rise in childhood overweight and obesity in the past decades. The number of overweight children has nearly tripled in the last 40 years, leaving the US with the disquieting figures of approximately 1 in 5 children (17%) now estimated to have obesity, while 16% are overweight.14,15 Exploring national data further, we can see that among children 2 to 5 years of age, obesity has more than doubled (from 5% to 13%), with similar increases experienced by 6 to 11 year-olds (from 7% to 19%). Among teens 12 to 19 years of age, obesity has nearly quadrupled from 5% to 21%.16
It is evident that two important questions must be addressed, swiftly and effectively:
- Why is the rate of overweight and obesity rising across the global population?
- What can be done to reduce current trends and prevent future increases across the globe, in all ages?
Reconsidering obesity… what are we missing?
In the past, most healthcare professionals and public health organizations in the weight loss field have delivered similar education and recommendations around the best purported methods to achieve and maintain a healthy weight: burn more calories than consumed by engaging in regular physical exercise and consuming a healthy, nutrient-dense diet. Additional recommendations approach obesity with a more multifactorial lens and may include things like: reduce or eliminate processed foods, obtain sufficient and restful sleep, limit stressors, address key macro- and micronutrient gaps, and support healthy gut microbiota.17,18 Nevertheless, the rates of obesity continue to rise globally. Further adding to the complexity of this trend is that increasing weight has not just been occurring in humans but has also been observed in pets, laboratory animals, and urban (wild) rats.8,19
A review of 24 populations representing eight different animal species living with or around humans in industrialized societies indicated that the trend of increasing body weight over time was positive; this included feral rodents, domestic dogs and cats, and primates and rodents living in research colonies, among others.19 These results seem to show that external factors, beyond caloric intake and adequate physical activity, are influencing the clear trend of weight gain and excess adiposity seen in both human and nonhuman mammals across the world.19 In fact, this information points toward the possibility that environmental factors, including obesogens, may be culprits in the multifaceted battle of the bulge as well.11
The short list of environmental factors that can contribute to weight balance includes:12 reduced access to physical activity resources or safe locations to exercise; food deserts (i.e., geographical areas lacking adequate, affordable, and nutritious foods); viruses; gut dysbiosis; social networks (i.e., increased risk of having obesity if an individual’s social or family circle has obesity); and obesogens.
Obesogens—where are they?
So where exactly are obesogens found in our day-to-day lives? Unfortunately, for most of the world, obesogens are omnipresent. There are several categories of obesogens that have been defined, which include:1,20,21
- Cigarette smoke
- Air pollutants—polycyclic aromatic hydrocarbons (PAH), PM 2.5
- Food additives—monosodium glutamate (MSG), high-fructose corn syrup (HFCS), nonmetabolizable sugars, etc.
- Household products, ex: cleaners and plastic/rubber compounds—acrylamide, phthalate, tributyltin (TBT), bisphenol A (BPA), parabens octylphenol, perfluorooctanoic acid (PFOA), triclosan
- Personal care products and cosmetic ingredients—PFOA, perfluorooctane sulfonate (PFOS), butylparaben, methylparaben, di(2-ehtylhexyl)phthalate (DEHP), dibutyl phthalate (DBP), triclosan
- Pesticides/fungicides—di(2-ethylhexyl)phthalate (DEHP), dibutyl phthalate (DBP), methylparaben, PFOA, triclosan, parathion, organophosphate pesticides (diazinon, chlorpyrifos), imidacloprid, triflumizole, zoxamide, quinoxyfen, fludioxonil, organochlorine pesticides (dichlorodiphenyltrichloroethane [DDT], hexachlorobenzene [HCB], lindane), pyrethroid pesticides (permethrin, deltamethrin), phenylpyrazole pesticide (fipronil), fungicide (pyraclostrobin)
- Flame retardants
- BPA and other byproducts/intermediate reactants—dioxin, acrylamide, TBT (organotin), benzo(a)pyrene
- Polychlorinated biphenyls (PCBs)
- Biogenic compounds—isoflavones, nicotine, permethrins
- Persistent organic pollutants (POPs) and other industrial additives such as phthalates
- Metals—lead, arsenic, cadmium
- Various pharmaceuticals (see Table 2)
The obesogen impact
Obesogens have been shown to create metabolic and hormonal disturbances within the animal or individual exposed to the compound(s).1,2,8,34 These mechanisms of action, which will be explored in the next section, can contribute to obesity and subsequent health problems in that animal or individual’s body over time, which is concerning.
Additionally, more recent research is showing that the obesogenic influence may spread beyond the exposed individual and have an impact that extends across generations—“transgenerational” effects—via the obesogens’ ability to alter DNA methylation and the expression of metabolism-relevant genes.22 This epigenetic influence by obesogens has been shown in animal models to impact up to four generations beyond the animal experiencing the initial exposure,22 truly giving rise to the need to understand how obesogens work and how to prevent their negative influence on, literally, the health and future of the world.
Obesogens—windows of susceptibility
Emerging literature suggests that obesogens, and EDCs overall, may exert deleterious effects at various times during the lifespan. However, there do appear to be critically sensitive windows in which obesogens might have the most effect both on the individual and in modifications that can span generations.23
The most sensitive time period is during fetal development and within the first few years of life.23 Additionally, preconception and peripuberty might also be important windows of susceptibility for exposure to obesogens.23 Obesogens’ ability to impact development is the point of intersection between the EDC and DOHaD fields.1,24
Obesogens—mechanisms of action and potential health effects
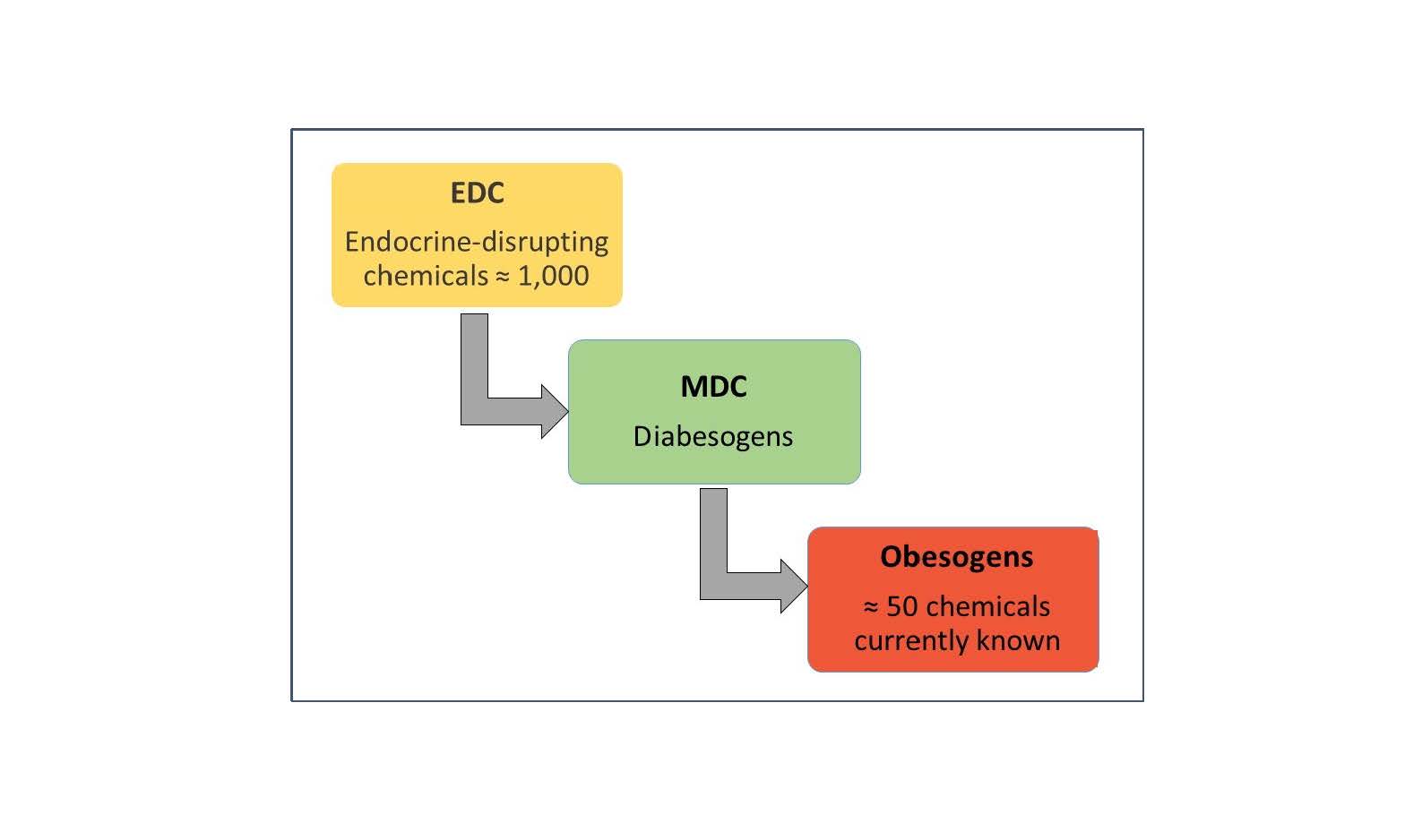
Unquestionably important to reducing obesogens’ impact on health is understanding how they work in the body and best ways to minimize and prevent exposures. Although the focus of this paper is to discuss obesogens, a subclass of the EDC category, it is important to mention that other subclasses of the larger EDC group (approximately 1,000 EDCs identified to date) have been implicated for their deleterious influences on metabolic disease including diabetes, NAFLD, and metabolic syndrome.23 This group of metabolically active toxins has been labeled “metabolism-disrupting chemicals” (MDCs) or “metabolism disruptors,” also called “diabesogens.”23 Figure 2 shows how these chemical categories are currently organized for research purposes:23,24
Figure 2: Organizational chart of environmental toxin categories23,24
Research has revealed diverse means by which EDCs, and obesogens in particular, can impart biological effects in the individual:7,22,24,25
- Increasing the number of adipocytes (increased quantity) by altering the metabolic set points
- Increasing storage in existing adipocytes (increased size)
- Impacting basal metabolic rate (BMR) to promote energy saving or calorie storing (“thrifty” phenotype)
- Modifying the signaling and receptor sites of appetite and satiety hormones (ghrelin, leptin, insulin, etc.)
- Modifying receptor activation of nuclear factors (retinoid X receptor [RXR], peroxisome proliferator-activated receptor gamma [PPARγ])
- Influencing endocrine system function (estrogenic, androgenic, and thyroid influences)
- Modifying epigenetic markers (transgenerational effects)
The obesogen field continues to grow, and much is still to be discovered, particularly since the bulk of the current research is preclinical, having been undertaken in animal models. However, there are a few key components that we know quite a bit about thanks to the increased focus and funding that have been directed toward this area—bringing evidence together from clinical work, public health sectors, and the environmental sciences.
Obesogens’ impact on fat tissue
Adipose tissue is a well-positioned target for obesogenic chemicals for a variety of reasons. First, adipose tissue is a dynamic organ dispersed throughout the body, creating an integrative network of communication linking energy metabolism, neuroendocrine, hormonal, and immune functions.7,26
Many of the known EDCs, particularly those linked to obesogenic influences, are highly lipophilic in nature, leading to the hypothesis that toxins can concentrate and accumulate within adipocytes.7 White adipose tissue (WAT) has been shown to be especially attractive to those environmental pollutants “which are resistant to biological and chemical degradation” or, more specifically in this case, persistent organic pollutants (POPs).27 It’s important to explore WAT as it pertains to obesogens. WAT provides insulation/heat and stores energy for use during increased need (starvation, high exertion, or any form of rapid weight loss).28 WAT also acts as a source for numerous metabolic and endocrine hormones including adiponectin, leptin, and resistin—all of which play a role in energy metabolism.28
When the body needs additional energy, various hormones bind to adipose cells, instigating the process of lipolysis or the release of energy-rich fatty acids and glycerol to be utilized in various tissues of the body.28 It’s thought that as these energy-rich molecules are released, accumulated EDCs might also be released into systemic circulation, potentially activating further downstream obesogenic interactions.7,28,29 In fact, loss of body weight in obese human subjects has been shown to increase plasma and subcutaneous adipose tissue concentrations of organochlorine pesticides and PCBs.30 For these reasons, it’s important that weight loss be undertaken in a slow, progressive manner, so the detoxification pathways and antioxidant status of the body are capable of handling the influx of previously sequestered toxins into systemic circulation.29
The inability to buffer and protect the body from a rapid release of EDCs from adipocytes during lipolysis could compromise health in several ways:
- Released obesogens may accumulate in other locations of the body, thus contributing to the weight gain cycle again and eventually leading to regain of the lost weight31
- Higher levels of POPs release during rapid weight loss may slow down or even reduce the overall benefits typically seen with weight loss30,31
- Some studies have shown that weight loss in obese individuals without comorbidities was linked to increased mortality when compared to obese subjects with stable weight.32 Might it be possible that this elevated risk comes from increased levels of released obesogens dumped into circulation and being redistributed into areas unable to mitigate their damaging effects?
Obesogens may also increase the risk of weight gain in the body through a chronic, low-level exposure from adipocytes that are “leaching” obesogens into systemic circulation;7 this may lead to similar outcomes as described above (i.e., exacerbation and perpetuation of weight loss/gain cycle and possibly further tissue damage).7
Obesogens’ impact on key nuclear hormone receptors
One particular area that has garnered much attention is the ability of obesogens to influence weight balance by targeting and binding certain nuclear hormone receptors.7 Research has shown that various obesogens such as tributyltin chloride and triphenyltin chloride (both chemicals are known EDCs) may activate RXR and PPARγ inappropriately, thus impacting lipid homeostasis and adipogenesis, including adipocyte differentiation activities.4
The downstream effects of erroneous nuclear hormone receptor activation depends on time of obesogen exposure. For example, exposure during the prenatal period may lead to a predisposition for obesity in adulthood, predominately manifesting in specific environments such as that of a high-calorie, high-fat Western diet.4
PPARγ is a well-studied factor in weight balance, as it is a key regulator of adipogenesis; when activated, it has been shown to stimulate fat cell development.33,34 It is hypothesized that many of the currently identified obesogens, in particular tributyltin, may increase adiposity and facilitate obesity through their actions on PPARγ.33,34 The role of PPARγ plays a critical part in multipotent stem cells by influencing the fate of the cell during adipogenesis; it’s thought that an obesogen’s ability to modify chromatin structure prior to cell differentiation can affect activation of PPARγ, thus biasing the multipotent stem cells toward increased adipogenesis and, quite possibly, increased risk of obesity in animals and humans.33
Recent studies indicate that activation of PPARγ by obesogens may also be working along alternative pathways. For example, PPARγ is the main target of the drug class of thiazolidinediones (TZD) (a potent insulin-sensitizing medication used to improve glycemic control in patients with type 2 diabetes), and TZDs are recognized obesogens, having been shown to lead to the proliferation of new fat cells.34 This increase in adipose tissue promotes obesity (and thus inflammation), thereby exacerbating the underlying risk factors associated with the very same condition the medication was meant to treat, diabetes.34
Obesogens’ impact on bone health
Research in a primary mouse bone marrow culture model has shown that the shift toward adipogenesis via obesogen influence via the activation of PPARγ may also suppress osteogenesis in bone marrow.35 Although more research is needed, this could ultimately translate into an environment highly primed for increased fracture risk, lower bone density, and higher risk of osteoporosis concurrent with the increased obesity risk.
Obesogens—other findings and emerging research
As discussed above, several well-documented mechanisms of action for obesogens have been put forth to the scientific community. However, more research in human subjects will be required to completely elucidate all the ways obesogens may be influencing the body and its biology. Below are some examples of obesogens’ influencing weight gain, although a complete understanding of the “how” are not yet fully available and will take more research and time.
- The odds ratio for obesity is approximately 2-fold in school-age children exposed to cigarette smoke before or during pregnancy.2,25,34,37 Animal studies indicate the mechanism might involve modulation of cholinergic and catecholaminergic systems by prenatal nicotine exposure.4
- Xenoestrogenic compounds in the environment (ex: BPA and nonylphenol) have been shown to promote adipocyte differentiation and/or proliferation of murine preadipocyte cell lines.34 It is unclear if these effects are via estrogen receptor signaling pathways only or if other mechanisms are involved.34 Most likely, “the nature of the effects may depend critically on the timing of exposure and the sex of the exposed individual.”34
- Obesogens, specifically POPs, have been shown to increase inflammation within adipocytes by upregulating the expression of inflammatory genes.36,38 In addition to increasing risk of obesity, this upregulated pathway also increases risk of metabolic disease processes.36,38
- Xenobiotic chemical exposure has been linked to increased body mass in human studies.25 Hexachlorobenzene present in umbilical cord blood has been associated with increased BMI in young children, regardless of mother’s BMI, while increased weight and BMI in adult female offspring has been linked to higher serum concentration of dichlorodiphenyldichloroethylene (DDE) in mothers.25
Medications with obesogenic effects
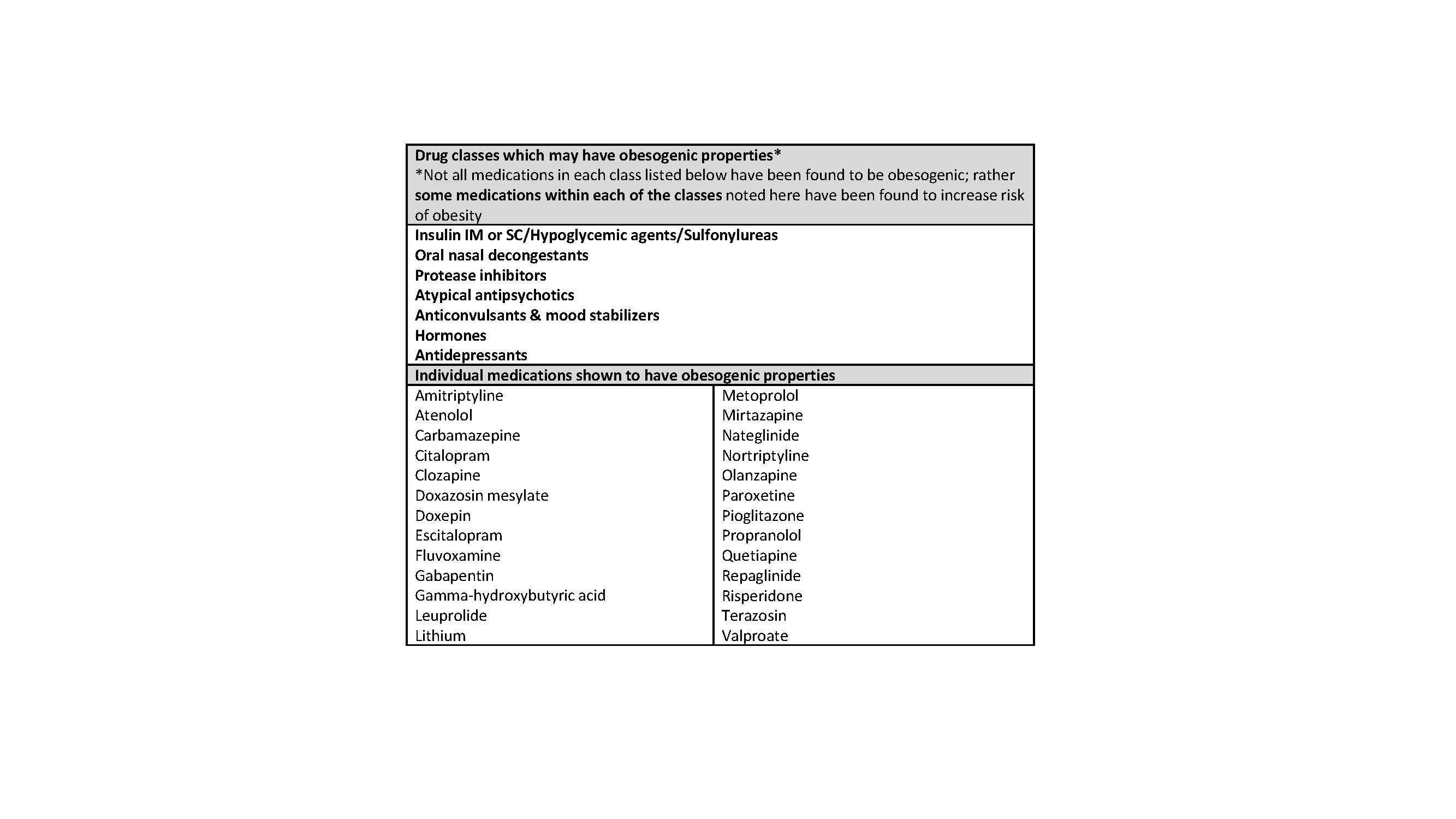
Certain pharmaceutical drug classes have been associated with increased body mass in humans.25
Table 2 provides a nonexhaustive list of medications with obesogenic effects.
Table 2: Drugs associated with weight gain25,39,40
Obesogens and the gut microbiome—a classic case of the chicken or the egg?
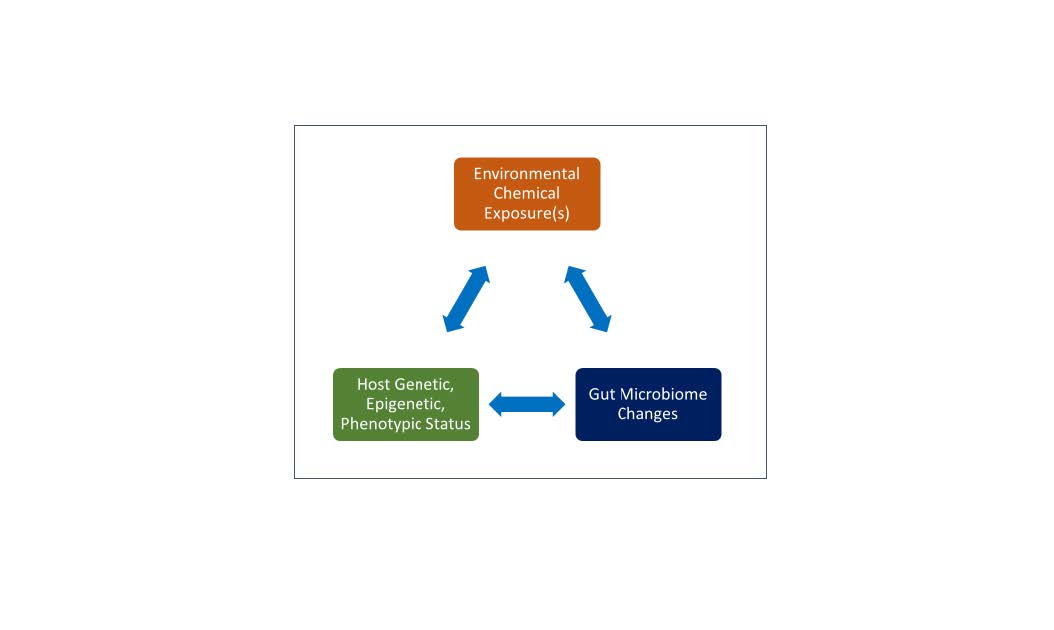
As Figure 3 depicts, it is not yet clear whether a change in the gut microbiome allows for increased deleterious effects from obesogenic exposures or whether the exposure to the obesogenic compounds alter the gut microbiome makeup.41 Further studies in both animal models and humans are needed to fully understand the important interactions at play. It may be found that there is a bidirectional effect among each of the three key components: environment, microbiome, and genetics.41
Figure 3: Bidirectional effects of environment, genetics, and gut microbiome41
Prevention & treatment approaches to offset obesogen exposure
A common-sense answer to the detrimental effects of obesogen exposure would be to “simply reduce exposure.” Unfortunately, in our current environment, very few locations on Earth are free of the toxic reaches of obesogens and EDCs at large. Exposure to obesogens occur through drink, diet, air, and touch; they are present in everyday foods, in water sources, and through inhalation of air contaminated by cigarette smoke and vehicle exhaust. They are present in furniture, nonorganic foods, baby toys, paint, and many other consumer products.

Obesogens can be inhaled, ingested, or absorbed transdermally. As can be deduced, these chemicals are ubiquitous; we literally eat, live, and breathe them every day. Reducing exposure might seem overwhelming, but small but intentional steps over time can reduce exposure. Additionally, supporting healthy and effective metabolic detoxification processes can help to metabolize and excrete obesogens.
Here are overarching concepts to highlight when attempting to reduce exposure to and effects of obesogens:
- Reduce overall exposure by identifying the most obvious routes and limiting interactions.
- The preconception period is an excellent time to support a “cleansing” of the bodies of the soon-to-be parents; it’s important to focus on optimizing all systems of the body, including detoxification organs and their pathways.
- Prenatal exposure is a major susceptibility window for exposure to obesogens; pregnant mothers should avoid as much contact with obesogens as possible during this time frame; however, never undergo a “detoxification” or intense weight loss protocol during pregnancy or while lactating.
- Weight loss efforts in the general population should be gradual to limit release of obesogens sequestered in adipose tissue into systemic circulation and hence, other organs.
- Detoxification or intense/acute weight loss while pregnant or lactating may increase EDCs’ entering the systemic circulation, resulting in a redistribution of obesogens potentially into areas that would increase the risk of exposure to the child (i.e., placenta, breast milk). During the prenatal time period, work with a personalize lifestyle medicine practitioner (e.g., Functional Medicine or naturopathic physician [ND]) to determine appropriate, targeted lifestyle steps; supplementation to support healthy detox pathways; and effective means to reduce obesogenic influences for both mother and unborn child.
More specifically, the exposure to obesogens can be reduced and mitigated through a number of practical, everyday tips:23,42-47
Food and beverage
- Eat a varied, colorful, and nutrient-dense diet
- Focus on fresh and frozen foods, and keep consumption of canned and processed foods to a minimum; in general, shop the “perimeter” of the grocery store
- Eating and cooking whole foods limits exposure to plastic packaging
- Utilize re-usable shopping bags
- Prepare and eat more meals from home; center them around fresh ingredients
- Eat organic when possible: Use the EWG’s “Dirty Dozen” and “Clean 15” lists42 as guidance for which foods to purchase organic vs. conventionally grown
- Eat foods that are locally grown and raised whenever available
- Avoid using straws, or opt for paper or glass straws
- Consult the Seafood Watch Consumer Guides43 or app by the Monterey Bay Aquarium for help in making the healthiest seafood choices for your body and the environment
- Trim fat from meat and remove skin from fish and poultry if these products are not grass-fed or wild (remember, toxins are stored in adipose tissue in animals as well)
- Eliminate consumption of sugar-sweetened beverages and MSG-containing products
- Eat a diet that is high in fiber, for example through fruits, vegetables, and whole grains like rice bran fiber (e.g., brown rice)
- Thoroughly wash fruits and vegetables in warm soapy water and with a brush before consuming them
- Use a high-quality water filter
- Drink water often and throughout the day. Avoid dehydration.
- Drink green tea
Storage & cooking
- Use glass, stainless steel, or porcelain storage containers
- Avoid plastic containers altogether
- Avoid putting hot foods or liquids into plastic containers
- Avoid use of nonstick cookware (e.g. pans)
- Use cast iron, glass, or stainless steel cookware
- Don’t microwave foods and beverages in plastic containers, including styrofoam products
- Is using plastic, look for BPA-free and BPS-free options
Personal care/hygiene
- Use soaps and personal hygiene items devoid of fragrances and antibiotics
- Avoid products with phthalates, parabens, and BPA
- Avoid all cosmetics that contain lead
- Consider adding a high-quality chlorine filter to showers and faucets
Daily activities
- Exercise and sweat regularly; avoid exercising in environments or conditions with heavy traffic, smog, or other air pollutants
- Limit contact with store/sales receipts—receipt paper and other thermal paper contain low levels of BPA; cashiers or others with frequent exposure should consider wearing gloves to reduce interaction47
- Opt for public transportation or carpool when possible; if distance permits, opt to ride a bike or walk
- Install high-quality air filters in home and vehicles; change regularly
- Limit vehicle idling
- Eliminate the use of pesticides
- Whenever possible, use “clean” household chemicals and yard/gardening products
- Consider wearing face mask (with filter) when cleaning, dusting, doing yardwork, etc.
- Do not smoke; avoid secondhand smoke exposure whenever possible
- Dust with a lightly dampened cloth regularly
- When possible, opt for non-toxic bedding and mattresses
- Replace pillows regularly and wash bedding often
- Avoid purchase of flame-retardant products in general and for home goods
- Consider alternatives to plastic toys, like wood
- Use paints with low volatile organic compounds (VOCs)
- Utilize electric over gas-powered tools and appliances when possible
- Add air cleansing plants indoors and plant trees and other foliage around house and in yard
- Avoid burning trash
Obesogens add an important piece to the puzzle for the growing obesity epidemic. The world of obesogen research is young and ripe for discovery. Emerging preclinical and clinical research will continue to add to our current understanding of EDC compounds. Clinicians are on the frontlines and are, therefore, uniquely positioned to inform patients of pragmatic ways to limit their exposure to obesogens.
Citations
- Heindel JJ. History of the obesogen field: looking back to look forward. Front Endocrinol (Lausanne). 2019;10:14.
- Baillie-Hamilton PF. Chemical toxins: a hypothesis to explain the global obesity epidemic. J Altern Complement Med. 2002;8(2):185–192.
- Grün F et al. Environmental obesogens: organotins and endocrine disruption via nuclear receptor signaling. Endocrinology. 2006;147(6 Suppl):S50-S55.
- UCI BioSci. Bruce Blumberg. https://devcell.bio.uci.edu/faculty/bruce-blumberg/ Accessed March 7, 2019.
- Zuo Z et al. Tributyltin causes obesity and hepatic steatosis in male mice. Environ Toxicol. 2011;26(1):79-85.
- Kassotis CD et al. Endocrine-mediated mechanisms of metabolic disruption and new approaches to examine the public health threat. Front Endocrinol (Lausanne). 2019;10:39.
- Regnier SM et al. Adipocytes under assault: environmental disruption of adipose physiology. Biochim Biophys Acta. 2014;1842(3):520–533.
- Holtcamp W. Obesogens: an environmental link to obesity. Environ Health Perspect. 2012;120(2):a62–a68.
- Kelly T et al. Global burden of obesity in 2005 and projections to 2030. Int J Obes (Lond). 2008;32(9):1431-1437.
- Wang Y et al. Will all Americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity (Silver Spring). 2008;16(10):2323-2330.
- Hu FB. Obesity Epidemiology. Oxford University Press; Oxford; New York: 2008:498.
- Hruby A et al. The epidemiology of obesity: a big picture. Pharmacoeconomics. 2015;33(7):673–689.
- CDC. The health effects of obesity and overweight. https://www.cdc.gov/healthyweight/effects/index.html Accessed March 12, 2019.
- CDC. Childhood Obesity Facts. https://www.cdc.gov/healthyschools/obesity/facts.htm Accessed March 8, 2019.
- Fryar CD et al. NCHS. Prevalence of overweight and obesity among children and adolescents aged 2–19 Years: United States, 1963–1965 through 2013–2014. https://www.cdc.gov/nchs/data/hestat/obesity_child_13_14/obesity_child_13_14.htm Accessed March 22, 2019.
- The State of Obesity. Childhood Obesity Trends. https://www.stateofobesity.org/childhood-obesity-trends/ Accessed March 7, 2019.
- IOM. Weight management: State of the Science and Opportunities for Military Programs. Chapter 4. Washington, DC 2004. https://www.ncbi.nlm.nih.gov/books/NBK221839/ Accessed March 12, 2019.
- John GK et al. The gut microbiome and obesity. Curr Oncol Rep. 2016;18(7):45.
- Klimentidis YC et al. Canaries in the coal mine: a cross-species analysis of the plurality of obesity epidemics. Proc Biol Sci. 2011;278(1712):1626–1632.
- NIEHS. Obesogens. https://www.niehs.nih.gov/health/topics/conditions/obesity/obesogens/index.cfm Accessed March 8, 2019.
- TEDX. The Endocrine Disruption Exchange. https://endocrinedisruption.org/ Accessed March 9, 2019.
- Chamorro-Garcia R et al. Ancestral perinatal obesogen exposure results in a transgenerational thrifty phenotype in mice. Nat Commun. 2017;8(1):2012.
- Sargis RM et al. Interventions to address environmental metabolism-disrupting chemicals: changing the narrative to empower action to restore metabolic health. Front Endocrinol (Lausanne). 2019;10:33.
- Heindel JJ et al. Environmental obesogens: mechanisms and controversies. Annu Rev Pharmacol Toxicol. 2019;59:89-106.
- Janesick A et al. Endocrine disrupting chemicals and the developmental programming of adipogenesis and obesity. Birth Defects Res C Embryo Today. 2011;93(1):34–50.
- Kershaw EE et al. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab. 2004;89(6):2548-2456.
- Müllerová D et al. White adipose tissue: storage and effector site for environmental pollutants. Physiol Res. 2007;56(4):375-381.
- Encyclopedia Britannica. Adipose tissue. https://www.britannica.com/science/adipose-tissue Accessed March 10, 2019.
- He F et al. Serum polychlorinated biphenyls increase and oxidative stress decreases with a protein-pacing caloric restriction diet in obese men and women. Int J Environ Res Public Health. 2017;14(1):E59.
- Kim MJ et al. Fate and complex pathogenic effects of dioxins and polychlorinated biphenyls in obese subjects before and after drastic weight loss. Environ Health Perspect. 2011;119(3):377-383.
- Cheikh Rouhou M et al. Adverse effects of weight loss: are persistent organic pollutants a potential culprit? Diabetes Metab. 2016;42(4):215-223.
- Chevrier J et al. Body weight loss increases plasma and adipose tissue concentrations of potentially toxic pollutants in obese individuals. Int J Obes Relat Metab Disord. 2000;24(10):1272-1278.
- Janesick A et al. Minireview: PPARγ as the target of obesogens. J Steroid Biochem Mol Biol. 2011;127(1-2):4–8.
- Grün F et al. Endocrine disrupters as obesogens. Mol Cell Endocrinol. 2009;304(1-2):19–29.
- Watt J et al. Structurally-diverse, PPARγ-activating environmental toxicants induce adipogenesis and suppress osteogenesis in bone marrow mesenchymal stromal cells. Toxicology. 2015;331:66-77.
- La Merrill M et al. Toxicological function of adipose tissue: focus on persistent organic pollutants. Environ Health Perspect. 2013;121(2):162–169.
- Al Mamun A et al. Does maternal smoking during pregnancy have a direct effect on future offspring obesity? Evidence from a prospective birth cohort study. Am J Epidemiol. 2006;164(4):317-325.
- Arsenescu V et al. Polychlorinated biphenyl-77 induces adipocyte differentiation and proinflammatory adipokines and promotes obesity and atherosclerosis. Environ Health Perspect. 2008;116(6):761–768.
- Domecq JP et al. Drugs commonly associated with weight change: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2015;100(2):363–370.
- Domecq JP et al. Drugs commonly associated with weight change: umbrella systematic review and meta-analysis (protocol). Syst Rev. 2012;1:44.
- Rosenfeld CS. Gut dysbiosis in animals due to environmental chemical exposures. Front Cell Infect Microbiol. 2017;7:396.
- EWG. Dirty Dozen, Clean 15. https://www.ewg.org/foodnews/ Accessed March 12, 2019.
- Seafood Watch. Consumers. https://www.seafoodwatch.org/consumers Accessed March 25, 2019.
- Crinnion WJ. How to live healthy in a toxic environment. https://www.naturopathic.org/content.asp?contentid=474 Accessed March 25, 2019.
- Sera N et al. Binding effect of polychlorinated compounds and environmental carcinogens on rice bran fiber. J Nutr Biochem. 2005;16(1):50-58.
- Chung RT et al. Detoxification effects of phytonutrients against environmental toxicants and sharing of clinical experience on practical applications. Environ Sci Pollut Res Int. 2017;24(10):8946-8956.
- Björnsdotter MK et al. Bisphenol A and replacements in thermal paper: a review. Chemosphere. 2017;182:691-706.
Sara Gottfried, MD is a board-certified gynecologist and physician scientist. She graduated from Harvard Medical School and the Massachusetts Institute of Technology and completed residency at the University of California at San Francisco. Over the past two decades, Dr. Gottfried has seen more than 25,000 patients and specializes in identifying the underlying cause of her patients’ conditions to achieve true and lasting health transformations, not just symptom management.
Dr. Gottfried is a global keynote speaker who practices evidence-based integrative, precision, and Functional Medicine. She recently published a new book, Brain Body Diet and has also authored three New York Times bestselling books: The Hormone Cure, The Hormone Reset Diet, and Younger.
Bianca Garilli, ND, IFMCP is a former US Marine turned Naturopathic Doctor (ND). Dr. Garilli works in private practice in Northern California and consults with naturopathic and Functional Medicine leaders, including the Institute for Functional Medicine and Metagenics. She is passionate about optimizing health and wellness in individuals, families, companies, and communities—one lifestyle change at a time. Dr. Garilli has been on staff at the University of California, Irvine, Susan Samueli Center for Integrative Medicine and is faculty at Hawthorn University. She is the creator of the Military and Veteran Health Initiative and is the current Past-President of the Children’s Heart Foundation, CA Chapter.




