


by Joseph Lamb, MD
“In 1982, while on sabbatical at the Linus Pauling Institute, I became convinced from the discussions I had with Dr. Pauling and many other luminaries that visited the Institute that the only way to really differentiate disease care from health care was through the development of a system that quantified health in terms of function and not the absence of disease.”
—Jeffrey Bland, PhD
President, Personalized Lifestyle Medicine Institute
We all likely agree with Dr. Bland that wellness is more than the simple absence of disease. It also is clear, when one awakens on a Monday morning with crushing chest pain while preparing for a busy day and subsequently receives a new diagnosis of coronary heart disease, that dysfunction has been ongoing and is now manifested as an ICD-10 diagnosis. To address the epidemic of noncommunicable chronic diseases, we must recognize this preclinical window of disrupted physiology and impending disease. The question rests in how best to do this, however.
The many recent advances in science and technology, including the recognition of the importance of systems-focused biology, have driven changes in the practice of medicine with an increasing focus on wellness. Hood, in describing P4 medicine has suggested that the best medicine should value four principles—medicine should be personalized, predictive, preventive, and participatory.1 Personalized care requires recognition of the uniqueness of the individual and the disease one has. Predictive care seeks to identify the preclinical trend/decline toward illness before the onset of symptoms that herald the loss of function and health through the gathering of unique patient-centered data sets. Preventive care utilizes the information gathered to intervene during the preclinical window to prevent disease. Participatory care requires engaging the patient in the healing relationship and recognizing the patient’s autonomy. Patients thus become active partners in gathering data to identify trends and apply lifestyle measures to improve their lives.
Discussing the challenges to utilizing these complex sets of individual patient data, however, Price has identified the lack of clear boundaries among disease, average health, and optimal wellbeing as a significant obstacle.2 Hanaway and Bland have discussed the usefulness of describing and measuring function to define these boundaries.3-4 In 2017, Bland, Minich, and Eck proposed using systems biology and unique functional assessments to improve the effectiveness of lifestyle medicine.5
Our group, here at the Personalized Lifestyle Medicine Center at Metagenics, is working to demonstrate that health indeed can be defined with functional measures of an individual’s capacities. Our recently published article in the Journal of Personalized Medicine, “Personalized Lifestyle Intervention and Functional Evaluation Health OUtcomes SurvEy: Presentation of the LIFEHOUSE Study Using N-of-1 Tent-Umbrella-Bucket Design,” describes our current clinical study.
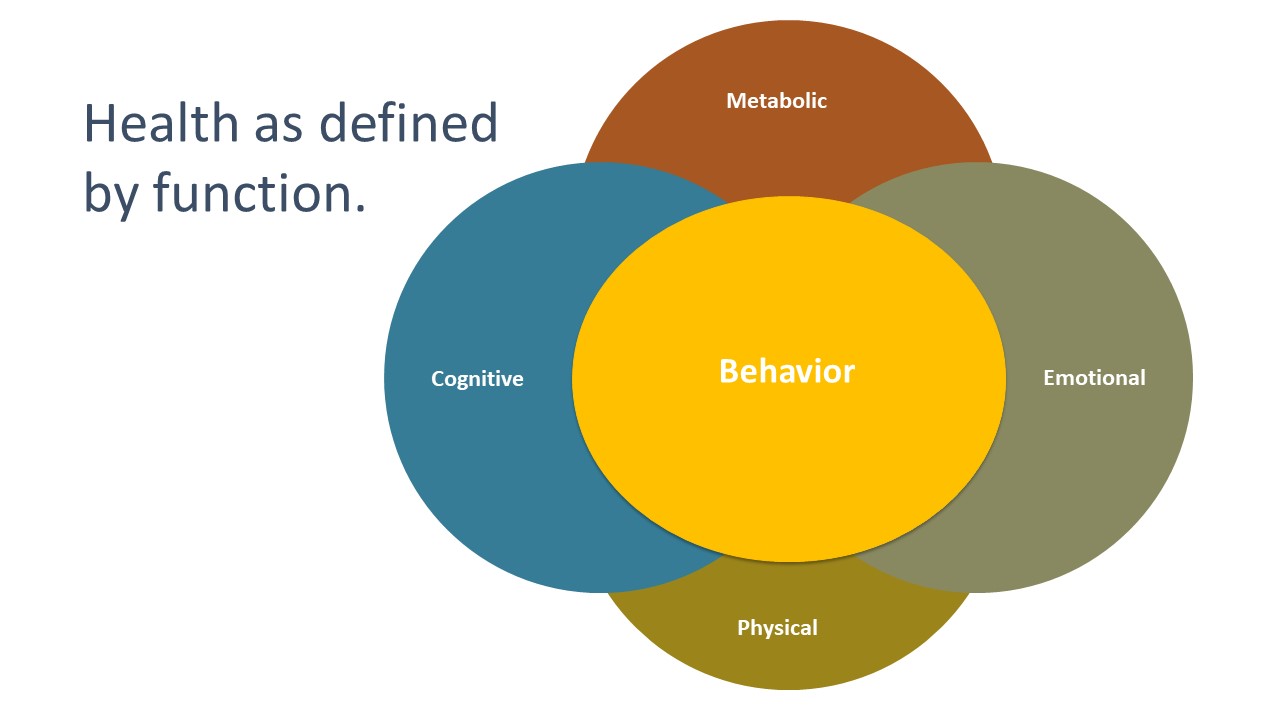
We have identified four functions, specifically metabolic, physical, emotional, and cognitive, which can be directly viewed, assessed, and quantified through the compilation and analysis of collections of deidentified, detailed patient histories, questionnaires regarding symptoms and general condition, and associated objective findings (genomic data, vital signs, and physical exam and laboratory biomarkers). Metabolic functions are assessed with standard laboratory biomarkers and imaging techniques. Laboratory evaluation include basic chemistries and blood counts, advanced lipid panels, inflammatory markers, nutritional markers, single nucleotide polymorphism analyses, and stool microbiome assessment. Measures of physical functions include expiratory peak flow, grip strength, balance, gait get up and go, bitter taste perception, and smell, as well as extensive anthropometric measurements and a nutrition-targeted physical examination. Cognitive and emotional functions can be well understood by selecting from the extensive array of available standardized questionnaires available to practitioners and researchers. Among the broad range of available questionnaires, the Rand MOS SF-36 Quality of Life assessment, measures of mood and stress (Depression Anxiety and Stress Scale, Beck Depression Inventory and Beck Anxiety Inventory), Patient-Reported Outcomes Measurement Information System (PROMIS) questionnaires, and the University of Rhode Island Change Assessment contribute to a deeper understanding of a patient’s uniqueness.
Our behavior is the fifth function—it is the expression of the activity and reserve in the other four functional capacities. Behavior reflects the choices we make each day—when to work, when to play, when and what to eat, when to fast, when to sleep, when and how to exercise, when to be alone, and when to be with others.
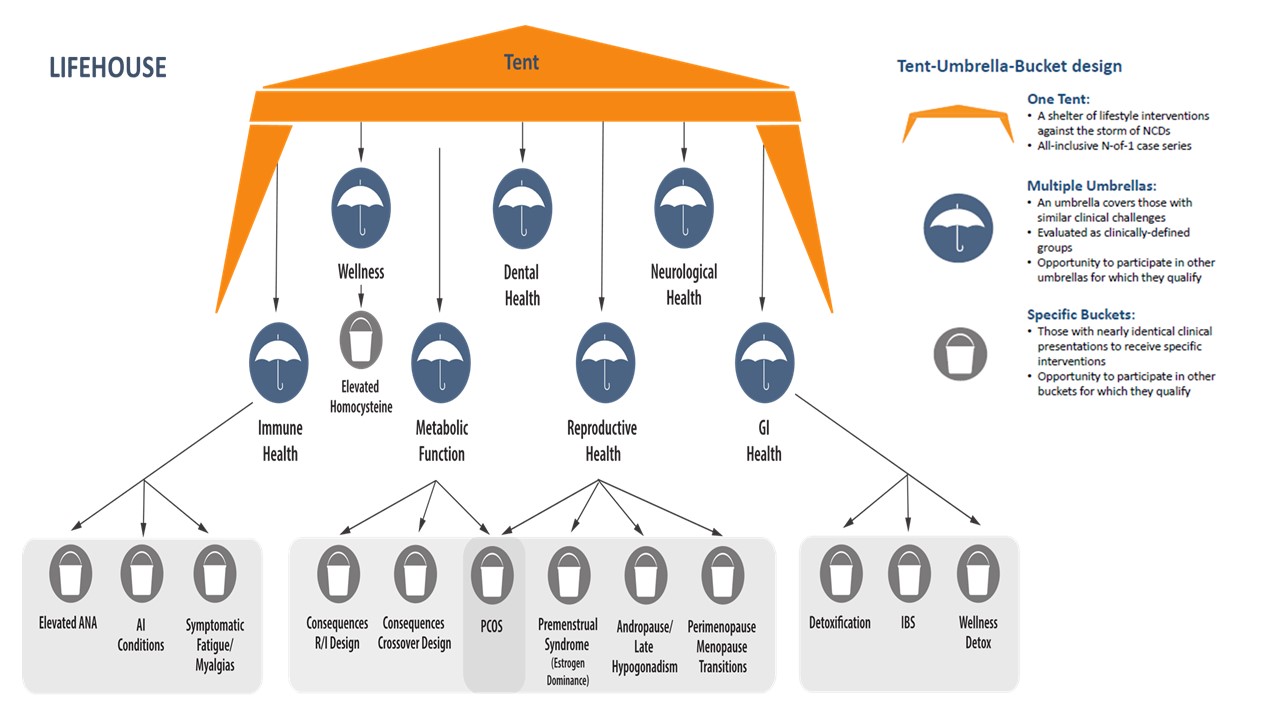
Personalized lifestyle medicine realizes the importance of these inputs and practices in creating programs to improve our health. LIFEHOUSE, as a personalized lifestyle intervention trial, uses an N-of-1 design, allowing for the creation of a program tailored to each participant based on individual metabolic, physical, cognitive, emotional, and behavioral needs determined through genomic analysis, medical history, and data sets of metabolic, microbiomic, physical, cognitive, emotional, lifestyle, and behavioral status. The aggregation and segmentation of data sets across the participant population can identify groups with similar clinical presentations yet segmented by genomic, microbiomic, and functional uniqueness. The N-of-1 designs addresses these uniquenesses with personalized lifestyle medicine recommendations and clusters these individuals according to shared similarities into several different subgroups (umbrellas, buckets) while still permitting analysis of entire group (tent).
LIFEHOUSE is a living, evolving study that continues to produce a wealth of exploratory opportunities related to our key research goals. This work currently has resulted in several planned papers exploring topics of interest including a polygenic risk score focusing on metabolic transformation/detoxification, assignment of individuals to umbrellas and thus personalized lifestyle medicine programs, and utility of a functional nutritional evaluation. Next steps include modifying the survey design and increasing both the diversity and amount of data available for analysis. Stay tuned.
Citations
- Hood L. Systems biology and p4 medicine: past, present, and future. Rambam Maimonides Med J. 2013;4(2):e0012.
- Price ND et al. A wellness study of 108 individuals using personal, dense, dynamic data clouds. Nature Biotechnology. 2017;35:747-756.
- Hanaway P. Form follows function: a functional medicine overview. Perm J. 2016;20(4):125-126.
- Bland J. Defining function in the Functional Medicine model. Integr Med (Encinitas). 2017;16(1):22-25.
- Bland JS et al. A systems medicine approach: translating emerging science into individualized wellness. Adv Med. 2017;2017:1718957.
Joseph Lamb, MD completed his graduate education at the Medical College of Virginia in Richmond, Virginia, and his Internal Medicine residency at Presbyterian University of Pennsylvania Medical Center in Philadelphia.
Dr. Lamb is doubly board-certified in Internal Medicine and Holistic Medicine/Integrative Medicine and is an Institute for Functional Medicine Certified Practitioner. With over 20 years of private practice experience, he is the co-owner and Medical Director of the Personalized Lifestyle Medicine Center by Metagenics in Gig Harbor, Washington. To date, he has been the Primary Investigator in over 75 clinical research studies.




