


By: Yekta Dowlati, PhD
The advent of GLP-1 receptor agonists (GLP-1 RAs) marks a transformative era in obesity and type 2 diabetes management. As of 2024, 6% of adults in the United States are currently using GLP-1 medications, with 12% reporting either current or previous use.1 Among those who have been diagnosed with overweight or obesity by a healthcare provider, this figure increases to 22%.1 These agents—such as semaglutide and tirzepatide—deliver clinically meaningful weight loss, improved glycemic control, and cardiovascular benefit in select populations.2 But as therapeutic use expands, so does our understanding of the complex physiological adaptations these drugs invoke. Among the most pressing concerns is the emergence of nutrient insufficiencies, driven not by malabsorption per se, but by profound reductions in energy intake and food variety.3 These deficiencies are not just theoretical: they are emerging in real-world practice, with measurable effects on energy levels, immunity, musculoskeletal health, and long-term metabolic outcomes.
For healthcare professionals, this represents a critical opportunity. Supporting patients through GLP-1 therapy isn’t just about achieving weight loss; it’s about preserving nutritional status, protecting lean mass, and sustaining resilience during a physiologically demanding process.3 Nutritional vigilance, including appropriate dietary counseling and targeted supplementation, is fast becoming a cornerstone of responsible GLP-1–based care.
Mechanisms That Suppress Appetite—and Nutrient Intake
GLP-1 RAs facilitates weight loss through several integrated mechanisms:2,4
- Delayed gastric emptying, prolonging satiety and reducing meal frequency
- Central appetite suppression, via hypothalamic and brainstem pathways
- Blunted hedonic drive, diminishing preference for energy-dense, palatable foods
- Glucose-dependent insulin secretion with concurrent glucagon suppression
While these mechanisms powerfully lower caloric intake—frequently driving consumption below 1,200 kcal/day in women and 1,800 kcal/day in men—they also indiscriminately reduce nutrient intake.3
Nutritional Deficits: A Predictable Outcome of Caloric Restriction
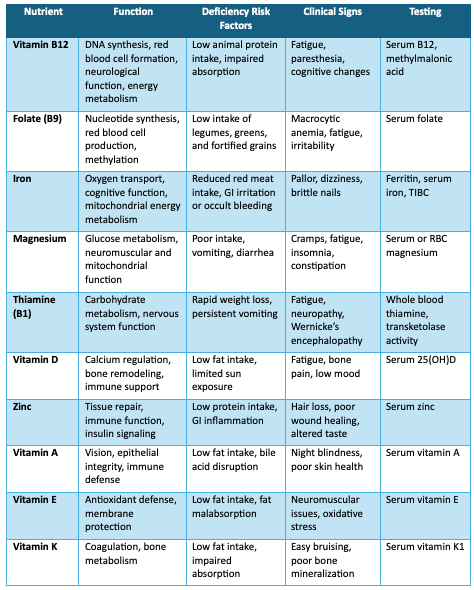
Sustained low energy intake inevitably creates a landscape where nutrient gaps are nearly unavoidable, particularly against the backdrop of already suboptimal baseline diets. In real-world observations, individuals on GLP-1 therapies often fall below dietary benchmarks for:3,5
- Microminerals: magnesium, potassium, calcium, iron, and zinc
- Vitamins: D, A, E, K, B12, B1 (thiamine), and folate
- Macronutrients: protein and fiber
- Phytonutrients: including carotenoids and flavonoids
Gastrointestinal effects—including nausea, bloating, early satiety, and evolving food aversions—further constrict intake variety and volume, amplifying the risk.
Clinical Monitoring: Identifying and Managing Risks
Proactive monitoring begins with a comprehensive dietary assessment, ideally supplemented by laboratory evaluations at baseline and within 3–6 months of therapy initiation.5-8 Recommended tests include:
- Vitamin B12 and methylmalonic acid
- Serum folate
- Ferritin, serum iron, and TIBC
- Serum or RBC magnesium
- 25-hydroxy vitamin D
- Serum zinc
- Whole blood thiamine or erythrocyte transketolase
- Vitamins A, E, and K1 in high-risk individuals
- Comprehensive metabolic panel for electrolyte status
In complex or refractory cases, advanced micronutrient testing from functional laboratories may be warranted.
The Clinical Consequences: Beyond the Scale
Unchecked nutrient deficits can subtly erode multiple systems, ultimately undermining the benefits of GLP-1 therapy. Potential clinical outcomes include:5
- Loss of lean body mass with reduced resting metabolic rate
- Compromised bone mineral density
- Anemia, fatigue, cognitive changes
- Impaired immune and antioxidant defenses
- Slowed detoxification capacity due to inadequate phytonutrient intake
Such cumulative effects not only threaten physiological stability but also diminish patient satisfaction, adherence, and long-term therapeutic success.
Building a Nutritional Strategy for GLP-1 Patients
To proactively support patients on GLP-1 receptor agonists, healthcare professionals should implement a multi-tiered nutritional strategy:
- Elevated protein intake is essential to counter anabolic resistance and protect lean mass. Aim for ≥1.2 g/kg/day, distributed across meals to optimize mTOR signaling. Patients struggling with reduced appetite may require strategic use of functional medical nutrition or protein-enhanced formulations.3,5
- Minimum safe caloric floors must be respected. Sustained intakes below ~1,200 kcal/day in women and ~1,500–1,800 kcal/day in men jeopardize not only muscle mass, but also endocrine, neurologic, and micronutrient homeostasis.5,9
- Micronutrient density is non-negotiable. Dark leafy greens, legumes, nuts, and seeds support magnesium, folate, and iron; fatty fish, eggs, and fortified dairy provide B12, vitamin D, and omega-3s; while diverse fruits and vegetables bolster antioxidant and phytonutrient defenses.3,5
- Hydration, Fiber, and GI Support:6 GLP-1 therapies may blunt thirst, increasing dehydration risks. Encourage above 2-3 liter of fluid per day,5 alongside 14 grams of fiber per 1,000 kcal,10 primarily from vegetables, legumes, and berries to sustain gut motility and microbial balance.
However, diet alone may not fully meet needs—especially under hypocaloric conditions.
A Role for Advanced Multi-nutrient Formulas
For patients unable to consistently meet nutritional needs through food—due to appetite suppression, GI intolerance, or time constraints—a broad-spectrum multi-nutrient supplement can serve as a foundational tool to bridge gaps and support metabolic health.
An ideal formula should offer:
- Methylated B vitamins (such as B12, folate)
- Chelated minerals (such as magnesium, iron, zinc)
- Vitamin D3, K2, and mixed tocopherols
- Carotenoids, flavonoids, and polyphenols
- Electrolytes (such as sodium, potassium, magnesium)
- Clinically validated antioxidant protection to counter oxidative stress
These formulations go beyond conventional multivitamins, targeting the nuanced needs of patients undergoing therapeutic weight loss. Their inclusion in care plans may help mitigate deficiencies before symptoms arise, preserve patient function, and improve quality of life throughout treatment.
The bottom line: sustaining weight loss by protecting what matters most
GLP-1 RAs are arguably the most potent metabolic tools we’ve seen outside surgery. But without parallel strategies to protect nutritional sufficiency, patients risk losing more than fat. They risk eroding the very foundation of their metabolic, immune, and neuromuscular resilience.
As stewards of long-term health, clinicians hold the responsibility to recognize the nutritional demands imposed by these therapies, and to address them through scientifically grounded, proactive strategies. Combining dietary guidance, resistance training, and comprehensive multi-nutrient support helps patients maximize the benefits of GLP-1 therapy while maintaining the nutrient status essential for sustained wellness.
References:
- Montero A et al. KFF Health Tracking Poll May 2024: The public’s use and views of GLP-1 drugs, Kaiser Family Foundation (KFF), 2021.
- Gul U et al. 2024;16(12):e76519.
- Mozaffarian D et al. Am J Lifestyle Med. 2025:15598276251344827.
- Moiz A et al. Am J Med. 2025;138(6):934-940.
- Almandoz JP et al. Obesity (Silver Spring). 2024;32(9):1613-1631.
- Christensen S et al. Obes Pillars. 2024;11:100121.
- Kesari A et al. In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 10, 2023.
- American Diabetes Association Professional Practice Committee. 2024. Diabetes Care;47(Suppl 1):S52–S76.
- Rippe JM. Am J Lifestyle Med. 2025:15598276251336677.
- Dahl WJ et al. J Acad Nutr Diet. 2015;115(11):1861-1870.




