


by Lewis Chang, PhD
Introduction
“Damned if I don’t get more tired every day. Tired of what I do. Following arcs, like lobbed rocks. The inevitability of truth. But the complexity and the grey lie not in the truth, but what you do with the truth once you have it.”—Detective Benoit Blanc (played by Daniel Craig, in the 2019 film Knives Out)
The current pandemic is not showing any sign of slowing in the US and many parts of the world. Nor is what scientists are learning. But the vast amount of information, much of it evolving, makes it difficult to digest. COVID-19 antibody testing is definitely a hot topic and a very confusing one.
My colleague recently asked: “If I test positive for antibodies but have never had symptoms, am I contagious, and do I have immunity?” It was such an important question but I soon recognized the complexity behind it. Maybe if I dissect the question into smaller ones, I could address it better. Let me start with:
What do coronavirus antibody tests measure?
Antibodies are proteins produced by our immune system in response to the presence of an antigen (AKA foreign substance, including pathogens such as SARS-CoV-2). Each antibody recognizes a specific antigen. It means an antibody to measles virus cannot recognize coronavirus, and an antibody to coronavirus cannot recognize measles virus. Antibodies aim to provide protection (immunity) when we are once again exposed to the same antigen by recognizing and latching onto the antigen and inactivating (neutralizing) it.
Humans have five different isotypes of antibodies; IgA, IgD, IgE, IgG, and IgM. Generally speaking, a COVID-19 antibody test measures the presence of two isotypes of antibodies to SARS-CoV-2 in the blood: IgM and IgG.1
- IgM is the first isotype of antibodies to develop during acute viral infection.2
- IgG is the predominant isotype found in the body and is responsible for long-term immunity after viral infection.2

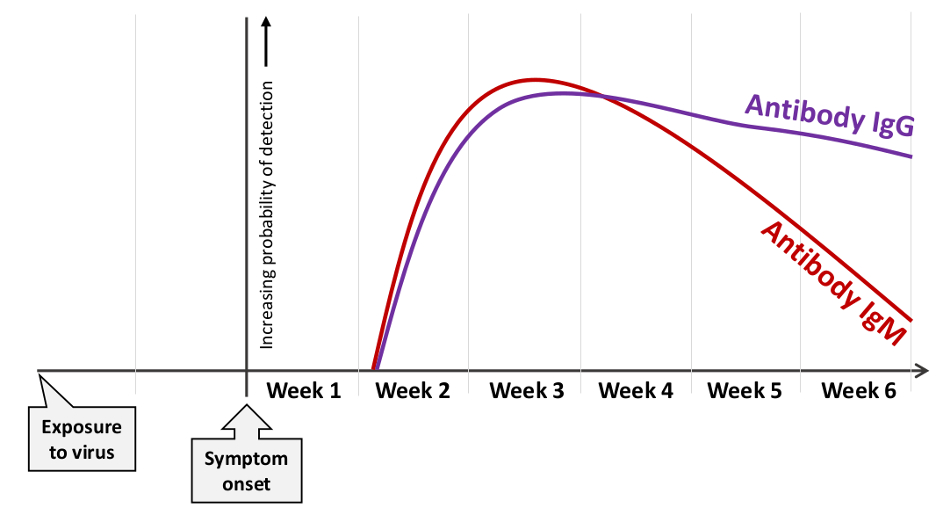
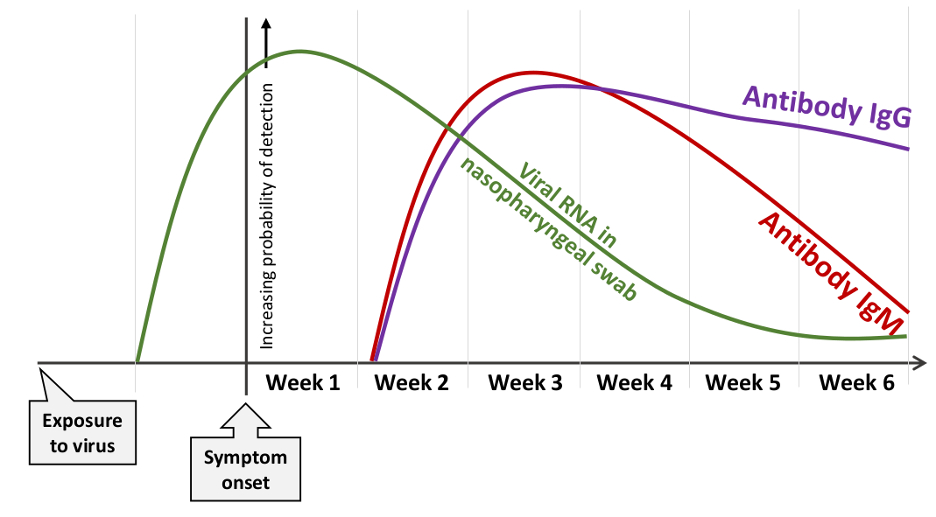
Early data tell us that antibodies to SARS-CoV-2 are not readily present within the first week after individuals experience symptoms of COVID-19, but then increase rapidly and become readily detectable the following two weeks, reaching their highest levels in the third week. As indicated in Figure 1, IgM and IgG may develop simultaneously or sequentially (IgM and then IgG). Afterward, IgM begins to decline whereas IgG remains present much longer.3 The trajectories in Figure 1 are rough estimates based on currently available but limited data. How quickly IgM drops and becomes undetectable can vary depending on the study and also the variability of IgM measurement. What has been observed in multiple studies is that IgG does not drop as quickly and will last at least several weeks (hence, longer-term immunity).4-6
How are these antibody tests done?
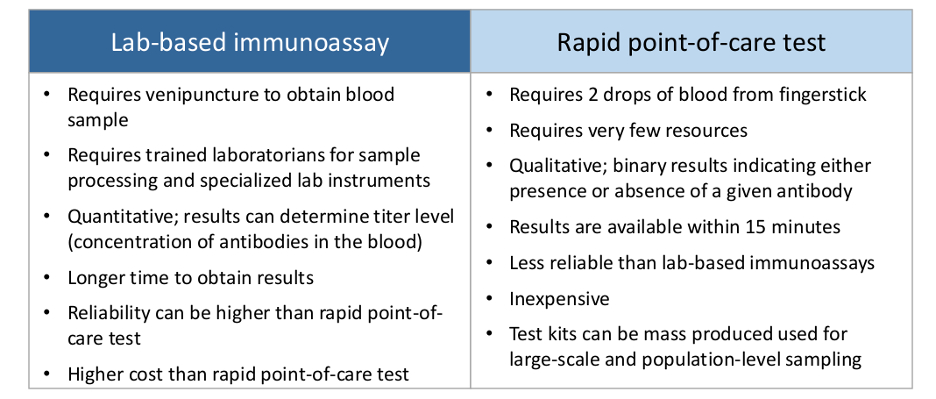
COVID-19 antibody tests are mainly done in one of two ways (Figure 2):1 a lab-based immunoassay [enzyme-linked immunosorbent assay (ELISA) or chemiluminescent immunoassay (CHIA)] or a lateral flow immunoassay (LFIA)-based rapid point-of-care test (with a disposable device, similar to a home pregnancy test).
What do the antibody test results mean, and how should test recipients act accordingly?
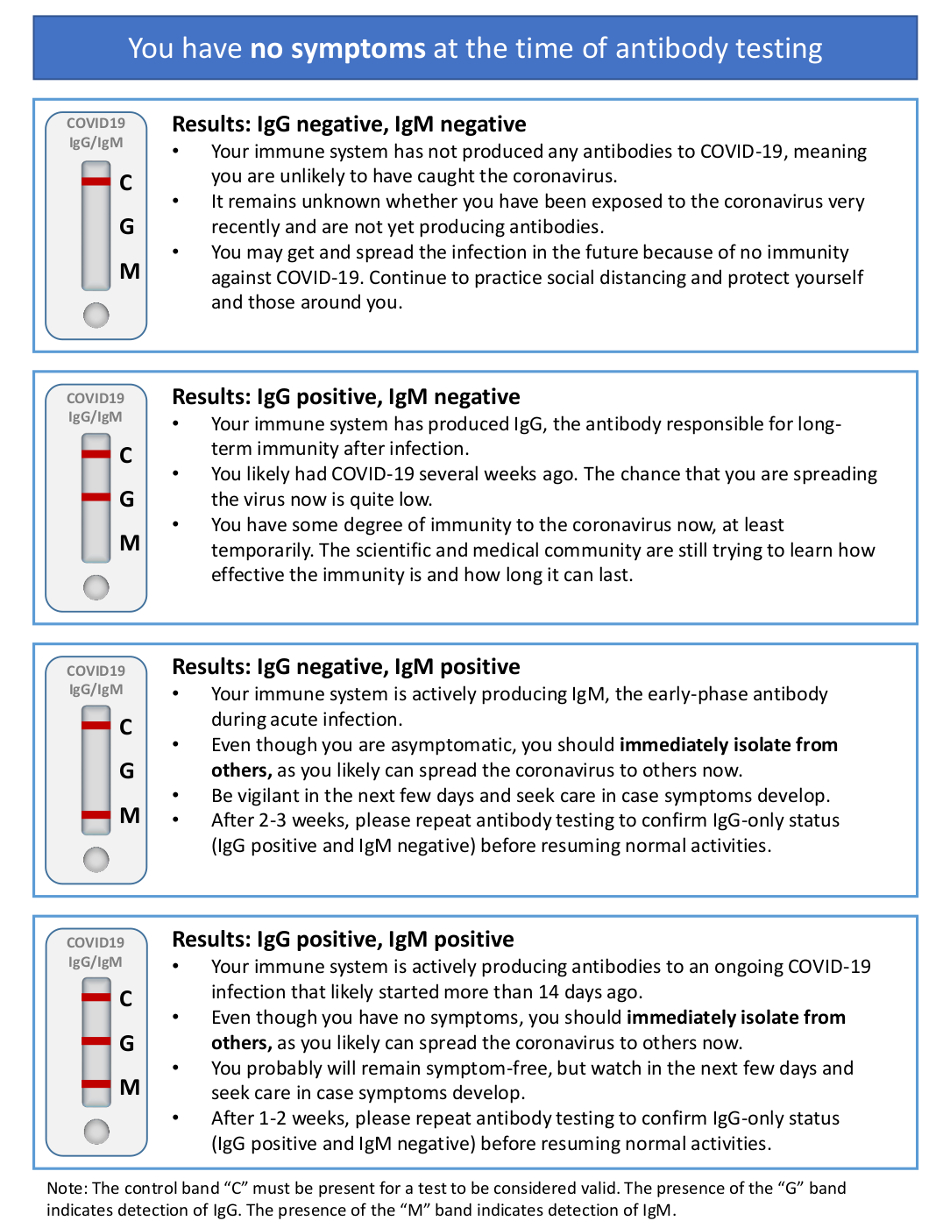
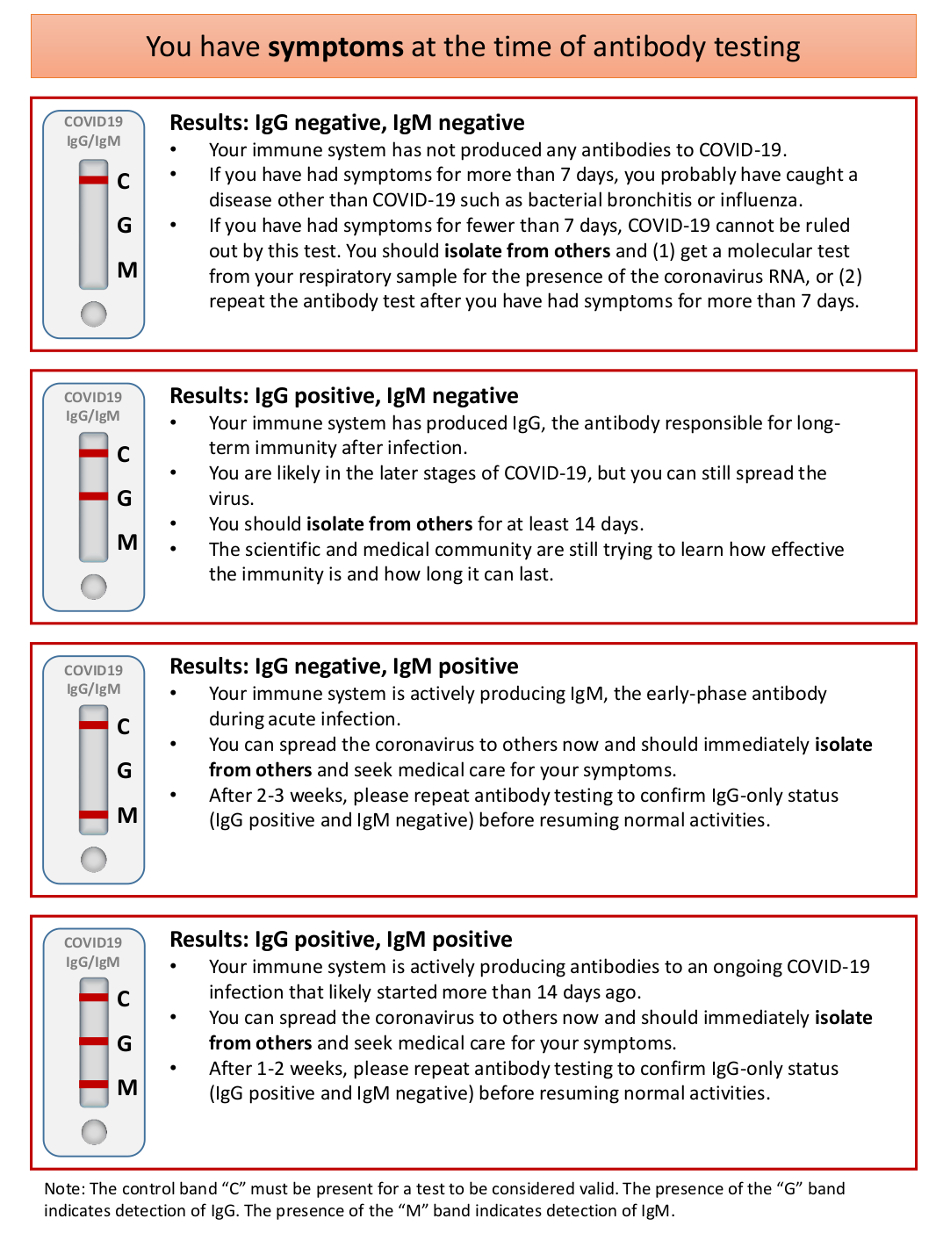
It would be helpful to interpret the test results by distinguishing whether the test recipient was symptomatic or asymptomatic at the time of testing. The result meaning and the recommended course of action are summarized in Figure 3a (for those who had no symptoms) and Figure 3b (for those who had symptoms).1 However, bear in mind that these antibody tests are not perfect (more on that later).
Are these antibody tests perfectly accurate?
Unfortunately, they are not. These tests have limitations and issues that can affect our confidence in the results just when we seek reassurance.
- Timing of testing
If an individual who really was infected with SARS-CoV-2 took an antibody test within a week after first symptom appeared, the test might or might not pick up the presence of antibodies, for the immune system was just starting to make antibodies. Testing conducted during this window would provide little certainty for test recipients.
- Accuracy of the test
As shown in Figure 1, seroconversion reaches the highest level around the third week after symptom onset, the ideal time to test for antibodies. Even so, tests conducted during that window are still not perfect.
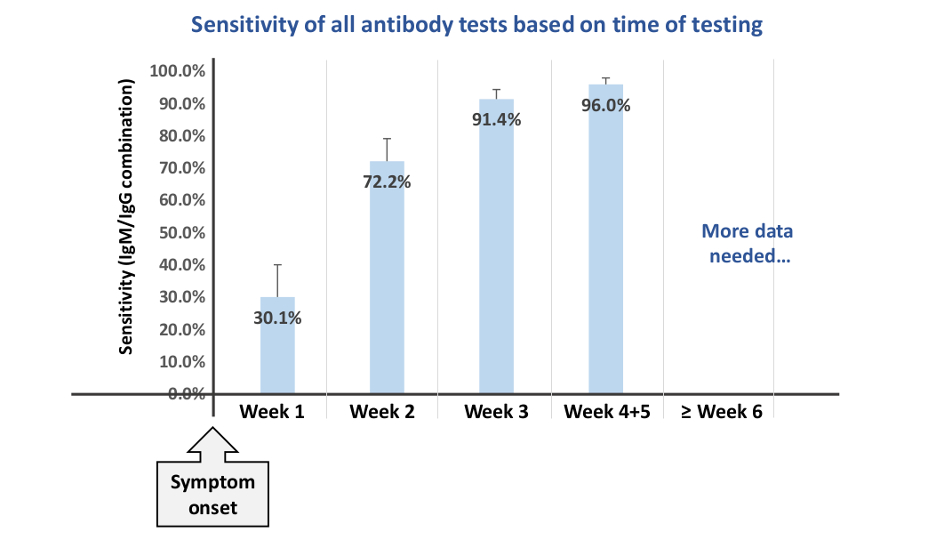
Cochrane Library (a global independent organization that systematically reviews research evidence of a given topic) recently conducted a large-scale analysis based on currently available evidence to understand the accuracy of COVID-19 antibody tests (Figure 4).7 Regardless of the quality of different test brands, the sensitivity—the ability of a test to correctly identify those who have antibodies to SARS-CoV-2 in the blood—of the test at the third week is on average 91.4%. In plain language, 91.4% of the individuals who have developed antibodies got the correct results (true positive), but 8.6% of the individuals who have developed antibodies ended up receiving a negative result. Without additional diagnostic tests to confirm their disease or antibody status, these individuals would think that they have never been exposed to SARS-CoV-2 when in fact they have.
The Cochrane review also analyzed the antibody test specificity—the ability of a test to correctly classify an individual as antibody-free when the individual truly has not developed antibodies. Regardless of the quality of different test brands and timing of the test, the specificity is on average 98%.7 In plain language, 98% of the individuals who had not developed antibodies got the correct results (true negative), but 2% of the individuals who had not developed antibodies ended up receiving a positive result (false positive).
- Cross-reactivity concerns
There are other coronaviruses in the world, including some that are responsible for the common cold. There are concerns that the antibody test designed to detect SARS-CoV-2 may pick up another coronavirus instead, leading to a false positive reading and misinterpretation of the result.
On the other hand, if an individual has antibodies to another human coronavirus, can those antibodies also recognize SARS-CoV-2 and confer protection to this individual? A preliminary report seems to have suggested such a possibility.8 In some healthy individuals who had never been exposed to SARS-CoV-2 but had a recent history of infection by human endemic coronaviruses (HCoV), their IgG against HCoV appeared to have SARS-CoV-2 neutralization activity.
It’s still too early to know for sure. Further, larger studies are definitely needed to know whether antibodies to a similar coronavirus can neutralize SARS-CoV-2.
If I have developed IgG, how long does the immunity last? Is there any chance of reinfection?
So far, there is no evidence showing people who have recovered from COVID-19 have become reinfected.9 This seems to suggest those people have developed functional immunity that is now protecting them. Or could it be once bitten, twice shy? Are these folks exercising extra precaution for fear of contracting it again?
COVID-19 has only existed in this world for a matter of months (it feels like it has been forever, though), not long enough to allow observation of longitudinal changes in IgG levels in relation to rates of reinfection. Absence of evidence is not the same as evidence of absence. We just haven’t gotten enough long-term data to argue either direction yet.
What we will probably get in the next several months are sensationalized news headlines that are based mostly on a steady stream of small, short-term studies (but every so often, there will be a larger, more robust longer-term study). For instance, in a small study of 74 Chinese individuals who recovered from COVID-19, researchers observed significant decreases in IgG levels within 2-3 months after infection.10 One headline wrote: “Study: Coronavirus antibodies could fade in just 2 months.” Another headline went: “Tom Hanks coronavirus: Could the actor get COVID-19 again?”
These studies, large or small, the results of which either in agreement or in conflict with one another, are all important in helping researchers piece together a bigger picture and shape our understanding of the current pandemic.
Conclusion
Another colleague of mine also posed an interesting question: “Is it worth the time and money to get tested if we still don’t know if it is possible to get COVID-19 twice?”
Antibody tests can potentially aid the diagnosis for COVID-19 for patients who may have passed the timing for reliable viral RNA detection. The PCR-based viral RNA test is the gold standard to confirm SARS-CoV-2 infection; however, it is known to be affected by sample type (for example, nasopharyngeal swab is less reliable compared with bronchoalveolar lavage specimen11), skill of the technician who collects the sample, and the timing of sample collection, resulting in missed diagnoses.12 As shown in Figure 5, Viral RNA detectability in nasopharyngeal swab starts to decline a week after onset of symptoms.3 Combining both has been shown to significantly increase the confidence of COVID-19 diagnosis.4
Antibody tests can yield knowledge that can guide the course of action for the test recipients (Figures 3a and 3b). The knowledge also helps researchers and public health experts develop and revise guidelines for social distancing, contact tracing, and the use of personal protective equipment—currently the primary methods to reduce spread of COVID-19.
Antibody tests can help identify individuals who have recently recovered from SARS-CoV-2 and have developed antibodies. These individuals are potential donors of convalescent plasma that are important for research in vaccine development and treatment development.
Antibody tests can provide information on the proportion of the population that has been exposed to SARS-CoV-2 and the portion of the population that remains susceptible to the coronavirus.
Antibody tests can help researchers identify whether some COVID-19 survivors fail to develop antibodies.
Antibody tests can identify whether someone may be at risk of inadvertently spreading the coronavirus because she or he never develops symptoms. In the first nationwide population-based study in Spain (one of the European countries most affected by the pandemic), researchers found that roughly a third of individuals who developed antibodies against SARS-CoV-2 were asymptomatic, corresponding to between 376,000 and 1,042,000 individuals.13
Yesterday I learned a new word: coronacoaster. Its definition is “the emotional ups and downs during the current pandemic. One day you are loving your bubble, doing yard work, baking banana bread and going for long walks, the next you are weeping, drinking gin for breakfast, and missing people you don’t even like.” In response, I will end with this:
“In a dark place we find ourselves, and a little more knowledge lights our way.”—Jedi Master Yoda
Citations
- Jacofsky D et al. Understanding antibody testing for COVID-19. J Arthroplasty. 2020;35:S74-S81.
- Schroeder HW et al. Structure and function of immunoglobulins. J Allergy Clin Immunol. 2010;125:S41-S52.
- Sethuraman N et al. Interpreting diagnostic tests for SARS-CoV-2. JAMA. 2020;323:2249-2251.
- Zhao J et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin Infect Dis. 2020. [Epub ahead of print].
- Long Q-X et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nature Medicine. 2020;26:845-848.
- Ma H et al. Serum IgA, IgM, and IgG responses in COVID-19. Cell Mol Immunol. 2020;17:773-775.
- Deeks JJ et al. Antibody tests for identification of current and past infection with SARS‐CoV‐2. Cochrane Database Syst Rev. 2020:CD013652.
- Ng K et al. Pre-existing and de novo humoral immunity to SARS-CoV-2 in humans. bioRxiv. 2020:2020.05.14.095414.
- Kirkcaldy RD et al. COVID-19 and postinfection immunity: limited evidence, many remaining questions. JAMA. 2020;323:2245-2246.
- Long Q-X et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nature Medicine. 2020. [Epub ahead of print].
- Wang W et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. 2020;323:1843-1844.
- Zou L et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382:1177-1179.
- Pollan M et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet. 2020. [Epub ahead of print].
Lewis Chang, PhD is Scientific Editorial Manager of R&D at Metagenics. Dr. Chang received his PhD in Nutritional Sciences at University of Washington, along with his MS in Nutrition and Public Health from Teachers College, Columbia University and BS in Pharmacy from National Taiwan University. Prior to joining Metagenics, he conducted dissertation research and completed a research assistantship and postdoctoral fellowship at the Fred Hutchinson Cancer Research Center in Seattle, WA. Dr. Chang has authored or co-authored and managed the publication of over 30 peer-reviewed journal articles and numerous scientific abstracts and posters. He has quite a green thumb, enjoys opera, theater and jazz, and loves cooking, collecting art, and learning to play gypsy jazz guitar.




