


For the past 40 years, clinical research in inflammation has been focused on blocking, suppressing or inhibiting an inflammatory response. This focus was largely driven by an interest to facilitate recovery, modulate a better immune response and to minimize or manage pain responses. And, while these approaches have resulted in symptomatic relief, unknowingly, blocking the inflammatory response resulted in suppression of an active process now known to fully resolve the inflammatory response. The outcome of this has since been shown to actually contribute to chronic inflammation with progression to chronic disease states.
Today, fortunately, we now know that an independent active process of resolution is required to bring about recovery from the inflammatory process. And as inflammation is an underlying cause of chronic disease, we now also know that if left unaddressed, inflammation cannot resolve itself and progression of chronic disease may in fact be accelerated. Recent studies have revealed when patients are deficient in their ability to resolve inflammation, there is a progression in chronic disease states – this deficiency has been described in an increasing number of chronic disease states including obesity or metabolic syndrome, diabetes, cardiovascular diseases, mild cognitive impairment, compromised digestive function (e.g., IBS, IBD, SIBO etc.), certain autoimmune conditions, Lyme disease, chronic obstructive pulmonary disease, arthritis (rheumatoid and osteoarthritic), and a variety of other chronic conditions often complicated by chronic pain. Managing the resolution of inflammation can be supported by critical lipid mediators known as specialized pro-resolving mediators (SPMs).
As underlying inflammation is the basis of chronic disease, it is critical to evaluate how resolution of inflammation can be effectively addressed and how specific care regimen options differ both in use and outcome. Below are some general clinical insights important to consider when creating a care program for patients with chronic disease.
SPMs and inflammation resolution
Inflammation is an immune response to insults such as injuries (e.g., cuts and wounds), infections (e.g., bacterial, viral or fungal), or unhealthy dietary patterns. The ideal outcome of inflammation is resolution and a return to homeostasis. Although an inflammatory response is an essential, protective response, it can give rise to chronic inflammation if left unresolved.1
After an inflammatory response is in progress, SPMs are produced to actively orchestrate activities during the resolution phase to accelerate the return to homeostasis. SPMs are essential in resolution activities, shutting down inflammation, expediting the complete return to homeostasis, and promoting tissue repair.2,3
SPMs are structurally different from omega-3 fatty acids
During the resolution phase of an inflammatory response, SPMs are biosynthesized (through multiple steps of enzymatic reactions) from long-chain polyunsaturated fatty acids and especially omega-3 fatty acids EPA and DHA.2,3 SPMs themselves are structurally different from omega-3 fatty acids.
SPMs are functionally different from EPA and DHA
EPA and DHA are important nutrients for health; EPA is especially good at lowering serum triglycerides.4,5 During the initiation phase of inflammation, potent pro-inflammatory mediators such as PGE2 and LTB4 are derived from arachidonic acid (AA). EPA and DHA themselves can affect the initiation phase by competing with AA for enzymes, leading to production of metabolites with lower biological potency than AA metabolites.6 EPA and DHA do not have the pro-resolving properties of SPMs.
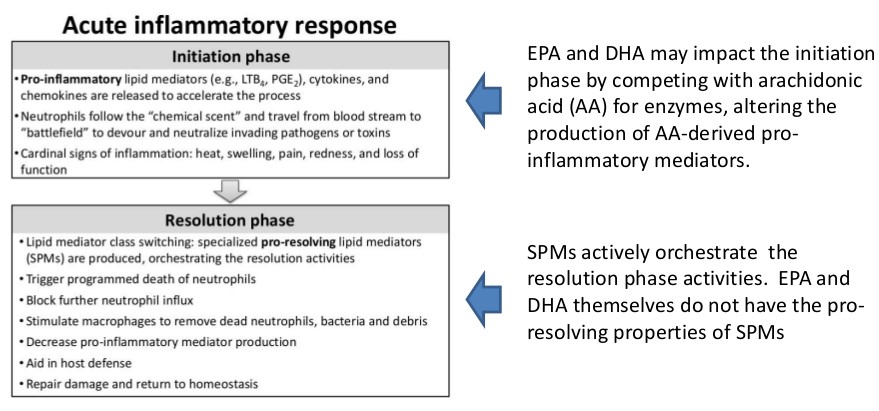
SPMs (not EPA and DHA) lead and orchestrate the resolution phase of inflammation
SPMs do not inhibit the initiation phase of inflammation. Rather, SPMs help facilitate the clearance of inflammatory components and thus resolve the inflammatory response. SPMs limit the further recruitment of neutrophils (immune cells) but stimulate the recruitment of pro-resolving macrophages that organize the clearance of inflammatory exudates containing microbes and dying neutrophils.3
To learn more about SPMs vs. fish oil, view the link below:
Fish Oils vs SPMs: What’s the Difference?
Direct supplementation is a more targeted approach
When inflammation is not resolved and becomes chronic, it is understood that cellular responses leading to resolution have failed. In these situations, and when there are many pro-inflammatory mediators resulting in chronic inflammation, the production of SPMs leading to resolution is compromised and inefficient. Recent studies discovered that some health conditions lead to deficiencies of SPMs. For example, in the experimental setting of obesity, the formation of SPMs is severely deregulated,7,8 and the enzyme that inactivates SPMs is markedly up-regulated.9 Although EPA and DHA are the substrates of SPMs, the biological effects of EPA and DHA are subject to multiple downstream metabolic checkpoints (e.g., receptors and enzymatic activities). Thus, researchers have suggested that direct supplementation of SPMs may represent a more targeted, effective approach than supplementing the parent omega-3 fatty acids, especially when chronic inflammation is already present.8
For additional information on the unique role of SPMs in resolving inflammation, view the video below:
Inflammation Resolution & SPMs: Video Animation
References
- Recchiuti A. Immunoresolving lipid mediators and resolution of inflammation in aging. J Gerontol Geriat Res. 2014;3:151.
- Serhan CN. A search for endogenous mechanisms of anti-inflammation uncovers novel chemical mediators: missing links to resolution. Histochem Cell Biol. 2004;122(4):305-321.
- Serhan CN. Pro-resolving lipid mediators are leads for resolution physiology. Nature. 2014;510(7503):92-101.
- Trikalinos TA et al. Effects of eicosapentanoic acid and docosahexanoic acid on mortality across diverse settings: systematic review and meta-analysis of randomized trials and prospective cohorts. Nutritional Research Series. 2012;4. Rockville, MD.
- Wang C et al. Effects of omega-3 fatty acids on cardiovascular disease. Evid Rep Technol Assess (Summ). 2004;(94):1-8.
- Calder PC. Omega-3 polyunsaturated fatty acids and inflammatory processes: nutrition or pharmacology? Br J Clin Pharmacol. 2013;75(3):645-662.
- Clària J et al. Diversity of lipid mediators in human adipose tissue depots. Am J Physiol Cell Physiol. 2013;304(12):C1141-1149.
- Spite M et al. Resolvins, specialized proresolving lipid mediators, and their potential roles in metabolic diseases. Cell Metab. 2014;19(1):21-36.
- Clària J et al. Resolvin D1 and resolvin D2 govern local inflammatory tone in obese fat. J Immunol. 2012;189(5):2597-2605.




