


by Mark Houston, MD and Sara Gottfried, MD
A precision and personalized medicine approach to dyslipidemia and dyslipidemia- induced cardiovascular disease—including high LDL cholesterol, elevated triglycerides, low high-density lipoprotein (HDL) and HDL function, and other related cardiometabolic conditions such as insulin resistance and metabolic syndrome—is completely different from the conventional medicine approach. In this article, we will review the major paradigm shift that has emerged in the past 10 to 15 years regarding HDL, which is best known for its ability to carry cholesterol from the blood vessel to the liver for redistribution, metabolism, and elimination. Strong experimental evidence suggests that HDL facilitates other cardioprotective effects in the body through various anti-inflammatory, antioxidative, antiapoptotic, anti-immune and antithrombotic processes. On the other hand, emerging data demonstrates that total HDL cholesterol does not represent the full story, because randomized trials aimed at raising HDL do not show benefit. The latest understanding regarding the management of HDL is that in order for HDL to have cardioprotective benefits, it must be functional. Loss of HDL function may negatively impact cardiometabolic health. New guidelines suggest that tests of HDL function provide more value than traditional total lipid testing and even more than advanced lipid testing of HDL size. Nutrition and nutraceutical supplements may be the most effective way to prevent, repair, and reverse the loss of HDL function that occur in patients. The main takeaway concept is that the heterogeneity of HDL structure, composition, size, HDL particle number (HDL-P), and function is much more important and valuable than the measurement of HDL-C alone to provide comprehensive analysis of the protective qualities of HDL cardiovascular disease. Instead, advanced lipid biomarker testing should include HDL size, HDL particle number, total HDL content, and ultimately reverse cholesterol transport (RCT) and cholesterol efflux capacity (CEC), which are measures of measure of HDL functionality, once they become commercially available.
Introduction
High-density lipoprotein (HDL) cholesterol plays a vital role in lipid biology and coronary heart disease (CHD) pathophysiology. However, a major paradigm shift is happening in the medical community regarding the role of HDL cholesterol in dyslipidemia and dyslipidemia-induced cardiovascular disease, especially CHD and myocardial infarction (MI). HDL is known for its ability to scavenge for and ferry LDL cholesterol away from the arteries and back to the liver for redistribution, metabolism, and elimination, as well as for its anti-inflammatory, antithrombotic, anti-immune and antioxidative activity. The prevailing dogma for the past 30 years was that high total HDL was cardioprotective, because it reflected better clearance of LDL. However, the emerging narrative is that HDL is far more heterogeneous than previously understood. In order for HDL to be cardioprotective, it must be functional.1 Furthermore, there are genomic, proteomic, and other compositional considerations. The main takeaway is that because of the heterogeneity of HDL, measurement of HDL-C alone does not provide a complete picture of the protective qualities of HDL vis-à-vis cardiovascular disease.
High-density lipoproteins (HDL) are complex nanoparticles with more than 80 associated proteins, phospholipids, cholesterol, and cholesteryl esters. See Figure 1 for the structure of HDL and its attendant functions.
Fig. 1
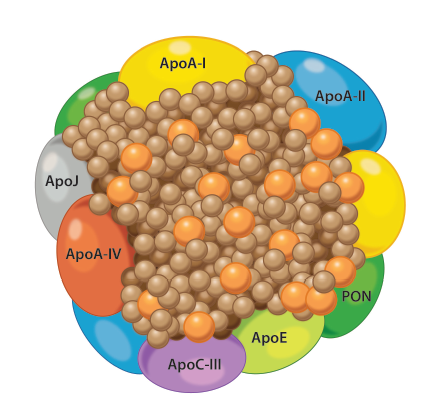
HDL: The paradigm shift about the role of HDL
Low-density lipoprotein (LDL) cholesterol is essentially a “garbage” type of lipid that deposits in cells all over the body, while the HDL is like a garbage collector. It literally takes LDL out of tissue to remove it from the body, usually through the liver.
Epidemiological studies, ranging from the Framingham Study2 and continuing through to the Atherosclerosis Risk in Communities (ARIC) Study,3 demonstrated that HDL is a consistently strong, independent risk factor for CHD and MI. Specifically, as the calculation was extended, CHD risk increases by 3% in men and 2% in women for every 1 mg/dL decrement in HDL.4 Put another way, patients were told that if you have good HDL, then you’ll have good “reverse cholesterol transport (RCT),” i.e., the body’s ability to clear LDL out of tissues. In the past, it was believed that as long as HDL levels were above a certain threshold, a patient was protected from having CHD and/or MI.
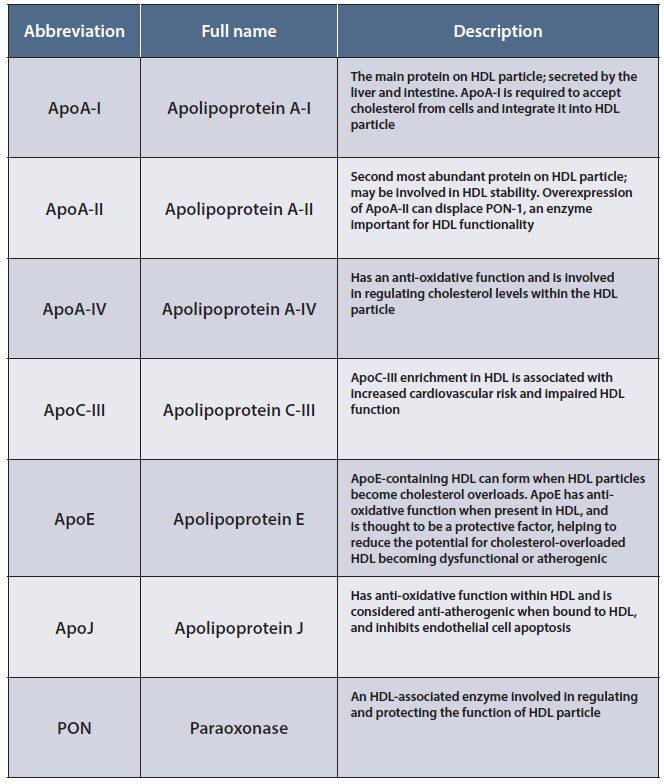
New research has updated that perception. Several threads of evidence point to a more nuanced model. Pharmacological interventions that raise HDL by two- to threefold have failed in randomized trials to produce the anticipated reduction in cardiovascular risk.5 Additionally, the level of the primary apolipoprotein associated with HDL, (apo) A-I, in HDL subtypes is a better predictor of cardiovascular risk than HDL-C concentration (Table 1).6 Further studies showed that the antiatherogenic capacity of HDL seems to be mediated by functionality, in this case, cholesterol efflux capacity, which is a superior predictor of risk than both Apo A-I concentration and total HDL-C concentration, though not all data are concordant.7 Further, data from genomewide association studies (GWAS) have shown that lower HDL-C may not cause CHD, that a high HDL may not be protective from CHD, and that heterogeneity of HDL structure and function may be more to blame.8
Table 1
In other words, if HDL is the garbage collector, there’s a range of options in the fleet. Some garbage trucks look good but don’t perform. Some have flat tires. But some of the garbage trucks are top of line, some have large carrying capacity and others have small carrying capacity, and others are highly dependable and perform beyond expectations. That’s the spectrum of HDL functionality.
We can no longer rely on high HDL for heart health protection, because experts are now questioning the composition and function of the various types of HDL.
What is HDL functionality?
Fig. 2
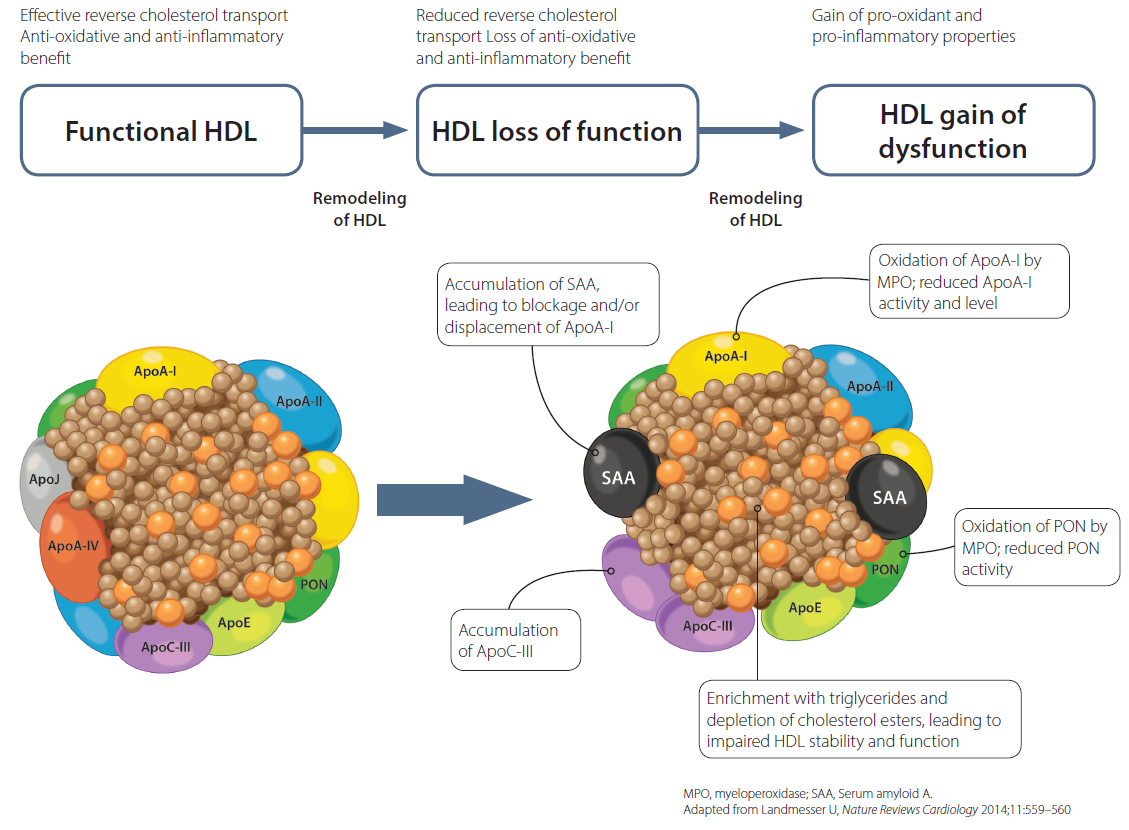

Static measurement of HDL-C fails to reflect the dynamics of the HDL particle, its remodeling process, the HDL load, HDL interconversions in the lipid pathway, the hepatic unloading, and resulting function.
Up until recently, HDL functionality could not be measured. We only had what were called “indicative markers of HDL functionality,” such as myeloperoxidase and some inflammatory and oxidative stress markers, but these were not the accurate assessors of HDL function. Thankfully, a revolutionary new test is now available that has the ability to measure RCT and CEC. This simple lab test will allow practitioners to accurately and effectively determine HDL functionality simply, though at the time of writing, this test is still in beta mode.
Investigators have demonstrated that assessment of CEC is one metric of HDL functionality and may in fact be a predictor of atherosclerosis and cardiovascular disease risk.9
New research is painting a broader picture that HDL function may be impaired in other situations of systemic inflammation oxidative stress and, such as autoimmunity, suggesting that improvement in HDL functionality may help beyond cardiovascular risk.10
HDL mapping of various subspecies of HDL
There are five different forms of HDL. The test used to measure these different forms is called “HDL mapping,” which includes α-1, α -2, α -3, α -4, and pre-β HDL. All of these forms are important; however, in the past the emphasis had been on the large HDL, which was α-1 in particular with a little bit of α-2. The concept has since changed. Some of the small particles, which are necessary to dock on the LDL tissue receptors and remove it, may be just as important in transforming to a larger HDL—which can handle more LDL, take it out, and deposit it in the liver. While the HDL size is important, it may be all types of HDL that play a role in this process.
But even size doesn’t matter without proper function. For example, a patient may have a normal level of all HDL sizes with the HDL mapping, but the HDL function may be abnormal. Think of it like a garbage truck with four flat tires. Although the garbage truck is large and potentially powerful, it won’t make it to its destination to complete its job (i.e., cleaning up LDL). That’s why functionality is the biggest key factor.
The importance of HDL particle number
The benefits of HDL also depend on the number of HDL particles. This is called HDL particle number, or HDL-P. Based on recent research, the higher the HDL particle number, the more protected you are from CHD and MI.11 That’s why many researchers agree that HDL function and particle number are the two most important factors when measuring HDL. In fact, in many studies the HDL-P and HDL function measurements are equally predictive of CHD and MI. If we’re able to determine both of these parameters together, we can better predict the role of HDL in providing protection from CHD and MI.
Testing 1, 2, 3
For any patient with a history of HDL-related problems, the first and most important step is to complete an advanced lipid profile, which will guide treatment options such as nutritional support, exercise, weight loss, and nutraceutical supplementation. This requires specialized labs—now available all over the United States—that determine all the previously mentioned parameters, including HDL size, HDL
Designing a nutritional medicine treatment protocol
Supplementation can play a key role in HDL management. Keep in mind, there are very few pharmaceutical agents that modify HDL. In fact, most won‘t affect the three parameters we’ve covered. However, various nutraceutical supplement and nutritional changes can modify at least one of these key factors.
- Pomegranate juice and pomegranate seeds have been shown to change some of the enzymes such as paroxonase (PON-1) in the HDL molecule and allow HDL to better transport LDL out of the cells.12
- Niacin shows promise for HDL-P and HDL support by improving function,13 though data are mixed.14
- Green tea extract, or EGCG, can also change the protein or lipid content of HDL so that the composition is not damaged by things like oxidative stress or inflammation, thereby reducing the risk of HDL dysfunction.15
- Increased intake of virgin olive oil, nuts, legumes, whole grains, and fish improves HDL functionality.16 Specifically, olive oil and whole-grain consumption raise CEC. More nut and legume intake improves paraoxonase-1 activity. Legume intake increases are also related to decreases in cholesteryl ester transfer protein activity. Fish consumption increments are associated with increases in paraoxonase-1 activity and declines in cholesteryl ester transfer protein activity, HDLcholesterol concentrations, and functions related to HDL levels (cholesterol efflux capacity).
- Anthocyanins consist of various soluble glycoside pigments that produce blue to red coloring in flowers and plants. Anthocyanin intake positive changes serum biomarkers related to HDL function in several patient populations, including dyslipidemia, hypertension, and diabetes, resulting in not only increased HDL cholesterol levels, but also HDL antioxidant and cholesterol efflux capacities.17
- HDL function may be improved by quercetin,18 glutathione,19 lycopene,20 resveratrol,21 and phosphatidyl serine22—alone or in combination, though several of the studies are underpowered, and more functional data are needed.23
Targeted nutritional therapy is associated with clinical benefit in various forms of dyslipidemia, including the use of red yeast rice, berberine, plant sterols or stanols (phytosterols), soluble fiber, citrus bergamot, flax seeds, and omega-3 fatty acids.
Track patient progress
The last piece of the puzzle is HDL mapping. When you complete an HDL map, you’ll find that some components may be in the red zone (not good), some in the yellow zone (borderline), or some in the green zone, which is great. Once you receive a patient’s results, you can institute or alter an existing supplement and lifestyle protocol to positively modify HDL and repeat testing in two to four months to track patient progress. Keeping a close watch and conducting follow-up tests is key and may require you to alter your recommendations as you see fit. Once a patient has achieved optimal levels of all three components, there should be a reduction in the event rate for CHD and MI.
For additional information, click here to watch Mark Houston, MD share the latest insights in HDL function and testing and how to formulate a precision and personalized protocol with diet and targeted nutraceuticals.
Conclusion: Support patients on the path to heart health
The latest discoveries on the key parameters of HDL efficiency have led to promising new treatment methods for better patient outcomes. Recognizing and measuring HDL type and size, functionality, and particle number are key factors in protecting patients from CHD and MIs. Through proper nutrition and lifestyle protocols, we can better protect our patient populations from the perils of heart-related health concerns.
Key takeaways
A personalized, precision, and integrative cardiovascular medicine approach to dyslipidemia—including advanced lipid testing with LDL, HDL, and VLDL particle size and number and HDL function related to RCT and CEC are required to determine CHD risk and then provide targeted prevention and treatment strategies. This is completely different from the conventional medicine approach.
In this article, we explored the major paradigm shift that has emerged in the past 10 to 15 years regarding HDL, which is best known for its ability to carry cholesterol from the blood vessel to the liver for redistribution, metabolism, and elimination.
HDL facilitates other cardioprotective effects in the body through various anti-inflammatory, antioxidative, anti-immune, and antithrombotic activity.
Emerging data demonstrates that total HDL cholesterol does not represent the full story, because randomized trials aimed at raising HDL do not show benefit.
Loss of HDL function may impact negatively cardiometabolic health.
We recommend performing on patients an advanced lipid profile, which will guide treatment options such as nutritional support, exercise, weight loss, and nutraceutical supplementation. This requires specialized labs—now available all over the United States—that determine all the previously mentioned parameters, including HDL size, HDL particle number, and total HDL content. Reverse cholesterol transport, a separate test, is conducted for HDL functionality and should be added to the advanced lipid testing labs once it’s available.
References
- Kontush A et al. Functionally defective high-density lipoprotein: a new therapeutic target at the crossroads of dyslipidemia, inflammation, and atherosclerosis. Pharmacol Rev. 2006;58(3):342-374. Riwanto M et al. Dysfunctional HDL: from structure-function-relationships to biomarkers. In: von Eckardstein A et al. High Density Lipoproteins: From Biological Understanding to Clinical Exploitation. (2015, Berlin Heidelberg New York: Springer), 337-366. Rosenson RS et al. Dysfunctional HDL and atherosclerotic cardiovascular disease. Nat Rev Cardiol. 2016;13(1):48-60. Kajani S et al. Unravelling HDL—Looking beyond the Cholesterol Surface to the Quality Within. Int J Mol Sci. 2018;19(7):E1971. Srivastava RAK. Dysfunctional HDL in diabetes mellitus and its role in the pathogenesis of cardiovascular disease. Mol Cell Biochem. 2018;440(1-2):167-187. Epub 2017 Aug 21.
- Gordon T et al. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med. 1977;62(5):707–714. [PubMed]
- Sharrett AR et al. Coronary heart disease prediction from lipoprotein cholesterol levels, triglycerides, lipoprotein(a), apolipoproteins A-I and B, and HDL density subfractions: The Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2001;104(10):1108–1113. Atherosclerosis Risk in Communities Study Group. [PubMed]
- Gordon DJ et al. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 1989;79(1):8–15. [PubMed]
- HPS2-THRIVE Collaborative Group. HPS2-THRIVE randomized placebo-controlled trial in 25 673 high-risk patients of ER niacin/laropiprant: trial design, pre-specified muscle and liver outcomes, and reasons for stopping study treatment. Eur Heart J. 2013;34(17):1279–1291. Barter PJ et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med. 2007;357(21):2109–2122. ILLUMINATE Investigators. [PubMed]AIM-HIGH Investigators. Boden WE et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365(24):2255–2267. [PubMed] Schwartz GG et al. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med. 2012;367(22):2089–2099. dal-OUTCOMES Investigators. [PubMed] Ferri N et al. Present therapeutic role of cholesteryl ester transfer protein inhibitors. Pharmacol Res. 2018;128:29–41. [PubMed] HPS2-THRIVE Collaborative Group. Landray MJ et al. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371(3):203–212. [PubMed]
- Ballantyne FC et al. High-density a nd low-density lipoprotein subfractions in survivors of myocardial infarction and in control subjects. Metabolism. 1982;31:433–437. Asztalos BF et al. High-density lipoprotein subpopulation profile and coronary heart disease prevalence in male participants of the Framingham Offspring Study. Arterioscler Thromb Vasc Biol. 2004;24:2181–2187. Asztalos BF et al. Value of high-density lipoprotein (HDL) subpopulations in predicting recurrent cardiovascular events in the Veterans Affairs HDL-Intervention Trial. Arterioscler Thromb Vasc Biol. 2005;25:2185–2191. Williams PT. Fifty-three year follow-up of coronary heart disease versus HDL2 and other lipoproteins in Gofman’s Livermore Cohort. J Lipid Res. 2012;53:266–272. Asztalos BF et al. High-Density Lipoprotein Particles, Cell-Cholesterol Efflux, and Coronary Heart Disease Risk. Arterioscler Thromb Vasc Biol. 2018;38(9):2007–2015. doi:10.1161/ATVBAHA.118.311117
- Khera AV et al. Cholesterol efflux capacity, high-density lipoprotein function, and atherosclerosis. N Engl J Med. 2011;364:127–135. Rohatgi A et al. HDL cholesterol efflux capacity and incident cardiovascular events. N Engl J Med. 2014;371:2383–2393. Saleheen D et al. Association of HDL cholesterol efflux capacity with incident coronary heart disease events: a prospective case-control study. Lancet Diabetes Endocrinol. 2015;3:507–513. Li XM et al. Paradoxical association of enhanced cholesterol efflux with increased incident cardiovascular risks. Arterioscler Thromb Vasc Biol. 2013;33:1696–1705.
- Navab M et al. HDL and cardiovascular disease: atherogenic and atheroprotective mechanisms. Nat Rev Cardiol. 2011;8:222–232. Helgadottir A et al. Variants with large effects on blood lipids and the role of cholesterol and triglycerides in coronary disease. Nat Genet. 2016;48:634–639.
- Favari E et al. High-Density Lipoprotein Functionality as a New Pharmacological Target on Cardiovascular Disease: Unifying Mechanism That Explains High-Density Lipoprotein Protection Toward the Progression of Atherosclerosis. Journal of Cardiovascular Pharmacology. 2018;71(6):325–331.
- Macpherson ME et al. Impaired HDL Function Amplifies Systemic Inflammation in Common Variable Immunodeficiency. Sci Rep. 2019;9(1):9427. Published 2019 Jul 1. doi:10.1038/s41598-019-45861-1
- Bostan M et al. Pleiotropic effects of HDL subfractions and HDL-associated enzymes on protection against coronary artery disease. Acta Cardiol. 2015;70(3):333-340. Khera AV et al. Cholesterol efflux capacity, high-density lipoprotein particle number, and incident cardiovascular events: an analysis from the JUPITER trial (justification for the use of statins in prevention: an intervention trial evaluating rosuvastatin). Circulation. 2017;135(25):2494-2504.
- Fuhrman B et al. Pomegranate juice polyphenols increase recombinant paraoxonase-1 binding to high-density lipoprotein: studies in vitro and in diabetic patients. Nutrition. 2010;26(4):359-366.
- Yvan-Charvet L et al. Cholesterol efflux potential and antiinflammatory properties of high-density lipoprotein after treatment with niacin or anacetrapib. Arterioscler Thromb Vasc Biol. 2010;30:1430–1438. Morgan JM et al. Effects of niacin and Niaspan on HDL lipoprotein cellular SR-BI-mediated cholesterol efflux. J Clin Lipidol. 2007;1:614–619. Franceschini G et al. Differential effects of fenofibrate and extended-release niacin on high-density lipoprotein particle size distribution and cholesterol efflux capacity in dyslipidemic patients. J Clin Lipidol. 2013;7:414–422.
- Khera AV et al. The addition of niacin to statin therapy improves high-density lipoprotein cholesterol levels but not metrics of functionality. J Am Coll Cardiol. 2013;62:1909–1910. Alrasadi K et al. Comparison of treatment of severe high-density lipoprotein cholesterol deficiency in men with daily atorvastatin (20 mg) versus fenofibrate (200 mg) versus extended-release niacin (2 g). Am J Cardiol. 2008;102:1341–1347.
- Basu A et al. Green tea supplementation affects body weight, lipids, and lipid peroxidation in obese subjects with metabolic syndrome. J Am Coll Nutr. 2010;29(1):31-40.
- Hernaez A et al. Increased Consumption of Virgin Olive Oil, Nuts, Legumes, Whole Grains, and Fish Promotes HDL Functions in Humans. Mol Nutr Food Res. 2019;63(6):e1800847. Epub 2019 Jan 15.
- Millar CL et al. Effects of Dietary Flavonoids on Reverse Cholesterol Transport, HDL Metabolism, and HDL Function. Adv Nutr. 2017;8(2):226–239. Published 2017 Mar 15.
- Rosenblat M et al. Reduced glutathione increases quercetin stimulatory effects on HDL- or apoA1-mediated cholesterol efflux from J774A.1 macrophages. Free Radic Res. 2014;48(12):1462-1472. Epub 2014 Oct 7. Ren K et al. Quercetin induces the selective uptake of HDL-cholesterol via promoting SR-BI expression and the activation of the PPARγ/LXRα pathway. Food Funct. 2018;9(1):624-635.
- Rosenblat M et al. Reduced glutathione increases quercetin stimulatory effects on HDL- or apoA1-mediated cholesterol efflux from J774A.1 macrophages. Free Radic Res. 2014;48(12):1462-1472. Epub 2014 Oct 7.
- McEneny J et al. Lycopene intervention reduces inflammation and improves HDL functionality in moderately overweight middle-aged individuals. J Nutr Biochem. 2013;24(1):163-168. Epub 2012 Jul 21. Vilahur G et al. Intake of cooked tomato sauce preserves coronary endothelial function and improves apolipoprotein A-I and apolipoprotein J protein profile in high-density lipoproteins. Transl Res. 2015;166(1):44-56. Epub 2014 Nov 25. Müller L et al. Lycopene and Its Antioxidant Role in the Prevention of Cardiovascular Diseases-A Critical Review. Crit Rev Food Sci Nutr. 2016;56(11):1868-1879. Thies F. Cardiovascular benefits of lycopene: fantasy or reality? Proc Nutr Soc. 2017;76(2):122-129. Epub 2016 Sep 9.
- Wang S. Novel insights of dietary polyphenols and obesity. J Nutr Biochem. 2014;25(1):1-18. Hunter PM et al. Functional foods and dietary supplements for the management of dyslipidaemia. Nat Rev Endocrinol. 2017;13(5):278-288. Epub 2017 Jan 30.
- Darabi M et al. Can phosphatidylserine enhance atheroprotective activities of high-density lipoprotein? Biochimie. 2016;120:81-86. Epub 2015 Jun 30. Darabi M et al. Phosphatidylserine in atherosclerosis. Curr Opin Lipidol. 2016;27(4):414-420.
- Riccioni G et al. Effectiveness and Safety of Dietetic Supplementation of a New Nutraceutical on Lipid Profile and Serum Inflammation Biomarkers in Hypercholesterolemic Patients. Molecules. 2018;23(5):1168. Published 2018 May 14.
Sara Gottfried, MD is a board-certified gynecologist and physician scientist. She graduated from Harvard Medical School and the Massachusetts Institute of Technology and completed residency at the University of California at San Francisco. Over the past two decades, Dr. Gottfried has seen more than 25,000 patients and specializes in identifying the underlying cause of her patients’ conditions to achieve true and lasting health transformations, not just symptom management.
Dr. Gottfried is a global keynote speaker who practices evidence-based integrative, precision, and Functional Medicine. She recently published a new book, Brain Body Diet, and has also authored three New York Times bestselling books: The Hormone Cure, The Hormone Reset Diet, and Younger.
Mark Houston, MD, MS, FAHA, FASH, DABC is a highly recognized cardiovascular and hypertension specialist, serving as a physician at St. Thomas West Hospital in Nashville, where he holds several leadership positions including Director of the Hypertension Institute and Vascular Biology, Medical Director of Clinical Research, and Section Chief for the Division of Nutrition. Dr. Houston cofounded the Hypertension Institute, which is one of the leading institutes in the US for hypertension treatment. An American Society of Hypertension (ASH) specialist and Diplomate of the American Board of Cardiology, Dr. Houston is also a Fellow of the American Society of Hypertension (FASH), the American Heart Association (FAHA), Internal Medicine (ABIM), American College of Nutrition (FACN) and Anti-Aging Medicine (ABAARM). Dr. Houston received his medical degree from Vanderbilt University. He also obtained two master’s degrees, in Human Nutrition and Metabolic Medicine and Human Nutrition, from the University of Bridgeport and University of South Florida, respectively.

![New HDL Cholesterol Concepts for Coronary Heart Disease [Full video]](https://www.metagenicsinstitute.com/wp-content/uploads/2020/01/HDL-Cholesterol-318x239.jpg "New HDL Cholesterol Concepts for Coronary Heart Disease [Full video]")



