


by Sara Gottfried, MD and Nilima Desai MPH, RD
Dynamic duos exist throughout culture: Batman and Robin. Thelma and Louise. They also exist in lifestyle medicine, because nutrients don’t fly solo. They interact often interdependently, act as cofactors in metabolic pathways, and compete for receptors. One example is how vitamin C helps you absorb more iron, like you find in red pepper hummus. Other examples are zinc and copper, vitamin B12 and folate, or even the combination of berberine and milk thistle, which may increase the efficacy of berberine. One nutritional bioactive may be more important than the other for a specific biochemical scenario, or more proven in the scientific literature, but when combined, there’s synergy. The sum is greater than the parts.
The nutritional duo increasingly under consideration is vitamin D and K and how the synergy between them may improve patient outcomes. We all know that vitamin D deficiency and insufficiency are common, as described in detail in this foundational article on vitamin D deficiency and why the problem persists. Additionally, nutrient gaps for vitamin K are common. In this article, we will cover the role of vitamin D versus K, the data favoring vitamin D3 over D2 for supplementation, and the role of vitamin K1 versus K2. We will conclude with the clinical takeaways for how to manage the pairing of vitamin D and K in your clinical practice.
Introduction
Vitamins D and K are both essential fat-soluble vitamins that are pleiotropic nutrients and have important clinical significance for the skeletal and cardiovascular systems and beyond—meaning they have benefits outside of just bone strength and metabolism.1
Vitamin D (ergocalciferol-D2 and cholecalciferol-D3) acts as a steroid hormone and plays a central role in many components of our skeletal and extraskeletal health, including calcium homeostasis, bone mineralization, and promoting immune and cardiovascular function.2
Vitamin K (phylloquinone-K1 and menaquinones-K2) is another group of essential fat-soluble vitamins and cofactors that are required for the production of several important proteins that are involved in calcium and blood coagulation homeostasis.3 Vitamin K also plays a central role in decreasing calcium accumulation in the smooth muscles of vascular walls.3
Research Highlights
|
Vitamin D2 vs. D3
The biochemical steps required for the activation of both D2 and D3 result in the same active metabolite, calcitriol (1,25[OH]2D), but research has shown differences between the two forms in raising the serum 25(OH)D levels, the best indicator of vitamin D status.7
A meta-analysis of 7 intervention studies (conducted in the US, Canada, UK, Australia, Denmark, and Italy) that included 1,016 participants aged 18-97 years with varying vitamin D doses (1,000-300,000 IU), treatment time periods (28d-24wk), and methods of administration (oral vs. intramuscular injections), demonstrated that vitamin D3 supplementation is more efficacious at raising serum D levels, producing a significant increase in serum 25(OH)D levels from baseline compared to vitamin D2.7
Another study involving 107 subjects tested the effects of supplementing with 2,000 IU/d of vitamin D2, D3, or placebo during an 8-week period on the serum concentrations of 25(OH)D, 25(OH)D2, and 25(OH)D3.8 In the vitamin D3 supplementation arm, the concentrations of 25(OH)D3 increased significantly from 16.6 ng/mL at baseline to 35.3 ng/mL after 8 weeks, whereas in the placebo group, 25(OH)D3 levels decreased from 15.8 ng/mL at baseline to 12.5 ng/mL after 8 weeks.8 In the group receiving vitamin D2, the 25(OH)D2 levels increased significantly, but the 25(OH)D3 levels decreased from 14.6 ng/mL at baseline to 6.7 ng/mL after 8 weeks.8 One of the possible explanations for this occurrence can be attributed to the possibility that D2 impairs hydroxylation of D3 in circulation.8 Therefore, based on these results, it can be concluded that vitamin D3 increased 25(OH)D more effectively than vitamin D2.8
The research investigation continues to fully elucidate the mechanisms underlying the relative potency of vitamin D3 vs. D2 supplements on 25(OH)D levels. In fact, dosing schedule (daily vs. bolus dosing) and gender may play mediating effects on the differences, in addition to difference in metabolism (e.g., speed of hydroxylation) and catabolism of D2 vs. D3.9
Vitamin K1 vs. K2
Vitamin K1: Transported principally to the liver and regulates cofactors that aid in coagulation of the blood.3
Vitamin K2 (MK-4, MK-7): Transported to extrahepatic tissues, such as bone and the vascular wall. It is a cofactor for carboxylase activity and facilitates the ɣ-carboxylation of bone-specific proteins such as osteocalcin (OC) and matrix Gla (MGP).3 OC takes calcium from the blood and binds it to the bone matrix, which in turn helps increase bone formation.10 MGP inhibits calcium precipitation in the matrix of the cartilage, vessel wall, and soft tissue, thus helping to prevent vascular and soft tissue calcification.3
Studies have compared the effects of vitamin K1 vs. K2 on blood coagulation factor and serum half-life of vitamin K and have found the impact of K2 to be greater than K1 for both.11
Proposed synergy between vitamins D and K: bone and cardiovascular health
- Animal and human studies have demonstrated that vitamin D helps stimulate the production of vitamin K-dependent proteins OC and MGP, which support bone mineralization and decrease vascular calcification.12
- Long-term supplementation of vitamin D can lead to increased production of vitamin K-dependent proteins. If the increased demand is not adequately supported through diet or supplementation, the proteins can remain uncarboxylated, which can lead to increased vascular calcification and lower BMD.12
- Excess supplemental calcium intake without the support of vitamin D and K can lead to increased calcium deposits in the vascular tissue instead of the bones.12
- Vitamin K2, when combined with vitamin D3, decreases bone resorption by inhibiting osteoclastic activity.13
- In clinical settings, both vitamins D and K have been found to downregulate proinflammatory cytokines (IL-6, TNF-α) and reduce oxidative stress.1 Inflammation and oxidative stress have been linked to osteoporosis and cardiovascular disease.1
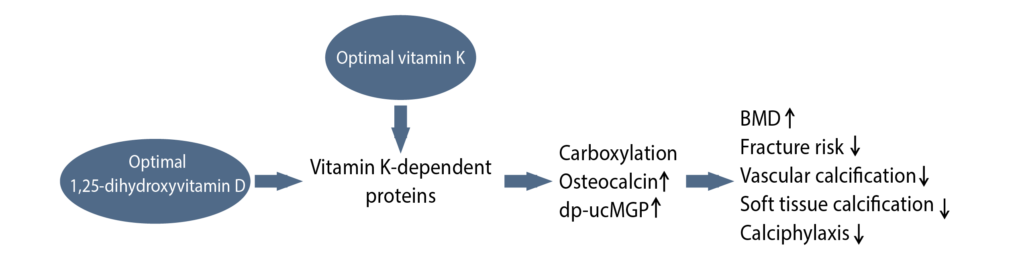
Image adapted from: van Ballegooijen AJ et al. Int J Endocrinol. 2017;2017:7454376.
Research
Bone mineral density
Study 1
A randomized controlled trial (RCT) involving 92 osteoporotic, postmenopausal women, aged 55-81 years, was conducted to assess the effect of the combined administration of vitamin D3 (as 1α-hydroxyvitamin D3) and K2 on bone mineral density (BMD) of the lumbar spine over a 2-year period.4 BMD was measured at baseline, 1 year, and 2 years. The participants were divided into 4 different groups:4
C Group: calcium lactate, 2 g/day
D Group: 1α-hydroxyvitamin D3, 0.75 mcg/day
K Group: vitamin K2, 45 mg/day
DK Group: 1α-hydroxyvitamin D3 + K2
This study demonstrated that BMD of the lumbar spine in osteoporotic women increased significantly with either the D3 (D group) or K2 (K group) administration (p<0.05 and p<0.001), whereas calcium (C group) administration resulted in BMD losses. Furthermore, the combined administration of D3 and K2 (DK group) produced even a higher increase in the BMD of the lumbar spine, compared to vitamin D3 and K2 interventions alone.
The mechanism for the beneficial impact of the combined administration of vitamins D3 and K2 remains unclear, and further studies are needed to understand this.
Study 2
Another RCT involving 126 postmenopausal women with osteopenia and osteoporosis was conducted to assess the effect of combined use of vitamins D3 (as 1α-hydroxyvitamin D3) and K2 on the vertebral BMD over a 2-year period.5 The participants were divided into the following 4 groups:5
Group 1: 1α-hydroxyvitamin D3 1mcg/day
Group 2: vitamin K2, 45 mg/day
Group 3: 1α-hydroxyvitamin D3 + K2
Group 4: control- dietary therapy alone
At the end of the study period, vertebral BMD decreased 4% in the control group, whereas it increased significantly in the group receiving combination therapy (D3 + K2) 4.92% ± 7.89%, p<0.01. Vertebral BMD increased 0.135% in the K2 group compared to control; the BMD result in the D3 group was significantly different from control but not from the K2 group.
Based on these data, it can be concluded that combination therapy may have a synergistic effect on improving vertebral BMD compared to D3 or K2 alone.
Study 3
An RCT involving 78 postmenopausal women aged 60+ was conducted to assess the effects of vitamins D and K on BMD and undercarboxylated OC (UcOC), a hip fracture indicator, over a 6-month period; 45 women completed the study and were included in the per protocol analysis.6
Vitamin D+K Group: 15 mg K2 3x/d, 400 IU D3 1x/d, 315 mg CaCO3* 2x/d
Control Group: 400 IU D3 1x/d, 315 mg CaCO3 2x/d
*CaCO3 = calcium carbonate
There was a statistically significant (p=0.049) increase in lumbar spine (L3) BMD in the vitamin D+K group compared to the control group. In addition, compared to baseline, the vitamin D+K group significantly decreased UcOC concentration (p≤0.01). UcOC also nonsignificantly increased in the vitamin D+K group.
Some observational and animal studies also support these findings.12 There were limitations to the study, including the small number of participants, high dropout rate, and lack of a separate comparator group that did not receive any supplementation.
Additional health benefits
Researchers are also studying the impact of joint supplementation of vitamins D and K on glucose metabolism and inflammation. These studies have demonstrated beneficial effects on markers of oxidative stress, upregulation of insulin receptor genes, and enhancement of β cell proliferation.12
Conclusion
Vitamins D and K represent common, significant nutrient gaps for the majority of Americans.14 Due to the synergy and overlap of these two nutrients in the regulation of calcium levels as well as the interplay in bone and cardiovascular health, the combination of D + K contributes to lower morbidity and mortality related to these conditions.1
Clinical takeaway: When you prescribe vitamin D to your patients for vitamin D deficiency or insufficiency, it is prudent to consider vitamin K, another common fat-soluble nutrient gap. Furthermore, the evidence to date for bone and cardiovascular health supports recommending vitamin D3 together with vitamin K2.
Citations
- Kidd PM. Vitamins D and K as pleiotropic nutrients: clinical importance to the skeletal and cardiovascular systems and preliminary evidence for synergy. Altern Med Rev. 2010;15(3):199-222.
- Kulie T et al. Vitamin D: An evidence-based review. J Am Board Fam Med. 2009;22(6):698-706.
- Schwalfenberg GK. Vitamins K1 and K2: The emerging group of vitamins required for human health. J Nutr Metab. 2017:6254836.
- Iwamoto J et al. Effect of combined administration of vitamin D3 and vitamin K2 on bone mineral density of the lumbar spine in postmenopausal women with osteoporosis. J Orthop Sci. 2000;5:546-551.
- Ushiroyama T et al. Effect of continuous combined therapy with vitamin K2 and vitamin D3 on bone mineral density and coagulofibrinolysis function in postmenopausal women. Maturitas. 2002:211-221.
- Je SH et al. Vitamin K supplement along with vitamin D and calcium reduced serum concentration of undercarboxylated osteocalcin while increasing bone mineral density in Korean postmenopausal women over sixty years old. J Korean Med Sci. 2011;26(8):1093-1098.
- Tripkovic L et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr. 2012;95(6):1357-1364.
- Lehmann U et al. Bioavailability of vitamin D2 and D3 in healthy volunteers, a randomized placebo-controlled trial. J Clin Endocrinol Metab. 2013;98:4339-4345.
- Hammami MM et al. Differential effects of vitamin D2 and D3 supplements on 25-hydroxyvitamin D level are dose, sex, and time dependent: a randomized controlled trial. BMC Endocr Disord. 2017;17(1):12.
- Maresz K. Proper calcium use: Vitamin K2 as a promoter of bone and cardiovascular health. Integr Med. 2015;14(1):34-39.
- Sato T et al. Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women. J Nutr. 2012;11:93.
- van Ballegooijen AJ et al. The synergistic interplay between vitamins D and K for bone and cardiovascular health: A narrative review. Int J Endocrinol. 2017;2017:7454376.
- Plaza SM et al. Vitamin K2 in bone metabolism and osteoporosis. Altern Med Rev. 2005;10(1):24-35.
- Fulgoni VL 3rd et al. Foods, fortificants, and supplements: Where do Americans get their nutrients? J Nutr. 2011;141(10):1847-1854.
Sara Gottfried, MD is a board-certified gynecologist and physician scientist. She graduated from Harvard Medical School and the Massachusetts Institute of Technology and completed residency at the University of California at San Francisco. Over the past two decades, Dr. Gottfried has seen more than 25,000 patients and specializes in identifying the underlying cause of her patients’ conditions to achieve true and lasting health transformations, not just symptom management.
Dr. Gottfried is a global keynote speaker who practices evidence-based integrative, precision, and Functional Medicine. She recently published a new book, Brain Body Diet and has also authored three New York Times bestselling books: The Hormone Cure, The Hormone Reset Diet, and Younger.
Nilima Desai, MPH, RD is Sr. Manager of Medical Marketing and Metagenics Institute. Nilima is a Registered Dietitian (RD) who received her undergraduate degree from California State University Long Beach in Nutrition and Dietetics and her Master’s in Public Health Nutrition from Loma Linda University. She has over 14 years of experience delivering medical nutrition therapy in the areas of diabetes, renal disease, weight management, and vegetarian nutrition. She also served on the board of the Renal Practice Group of the Academy of Nutrition and Dietetics from 2012-2016 as the Membership Chair. In her free time she runs half marathons and shuttles her two kids to their activities.




